Diabetic kidney disease (DKD) represents a major global health burden, yet predictive models often overlook socio-economic determinants that may independently influence disease progression. This retrospective cohort study aimed to identify socio-economic, demographic, and clinical predictors of diabetic kidney disease development among diabetic patients in Kenya and compare Cox regression with support vector machine (SVM) models for risk prediction. Data were collected from 756 adult diabetic patients attending Meru Teaching and Referral Hospital and Kerugoya Level 5 Hospital between January 2018 and July 2024 through medical record review and semi-structured questionnaires. Survival analysis employed Kaplan-Meier estimation, log-rank tests, multivariable Cox proportional hazards regression, and survival SVM modeling. During follow-up, 286 participants (37.8%) developed diabetic kidney disease. Multivariable Cox analysis identified seven significant predictors of diabetic kidney disease progression: older age at diabetes diagnosis (adjusted HR=1.023, p=0.002), male gender (HR=1.282, p=0.041), family history of chronic kidney disease (HR=6.919, p<0.001), alcohol consumption (HR=1.556, p=0.001), and financial hardship (HR=4.524, p<0.001) increased risk, while secondary/higher education (HR=0.593, p<0.001) and ever being employed (HR=0.635, p=0.011) were protective. The SVM model demonstrated marginally superior predictive accuracy (C-index=0.775) versus Cox regression (C-index=0.770). These findings underscore that socio-economic factors function as independent risk modifiers beyond traditional clinical parameters, challenging conventional prediction paradigms that focus exclusively on biomedical indicators. The high incidence of diabetic kidney disease observed highlights an urgent public health challenge requiring integrated screening protocols that assess both clinical and socio-economic risk profiles at diabetes diagnosis. We recommend implementing targeted public health interventions that address financial barriers, promote educational attainment, and support employment opportunities for diabetic patients to mitigate diabetic kidney disease progression in resource-limited settings.
| Published in | American Journal of Theoretical and Applied Statistics (Volume 15, Issue 2) |
| DOI | 10.11648/j.ajtas.20261502.11 |
| Page(s) | 27-39 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Diabetic Kidney Disease, Socio-economic Predictors, Survival Analysis, Cox Proportional Hazards Model, Support Vector Machine, Risk Prediction
Statistic | Time (years) | Patients age | Weight (Kgs) |
|---|---|---|---|
Mean | 12.14 | 41.29 | 83.98 |
Standard Deviation | 6.91 | 11.81 | 10.82 |
Median | 12 | 41 | 85 |
Range | 30 | 61 | 60 |
Skewness | 0.12 | 0.23 | 0.05 |
Kurtosis | -1.04 | -0.58 | -0.17 |
Maximum | 31 | 76 | 116 |
Minimum | 1 | 15 | 56 |
Feature | Frequency | (%) | |
|---|---|---|---|
Gender | Female | 396 | 52.4% |
Male | 360 | 47.6% | |
Hypertension | No | 270 | 35.7% |
Yes | 486 | 64.3% | |
Cardiovascular Diseases | No | 550 | 72.8% |
Yes | 206 | 27.2% | |
Education | Primary | 252 | 33.3% |
Secondary | 278 | 36.8% | |
Tertiary | 226 | 29.9% | |
Marital status | No Spouse | 388 | 51.3% |
Spouse | 368 | 46.7% | |
Tobacco use | No | 494 | 65.3% |
Yes | 262 | 34.7% | |
Alcohol use | No | 498 | 65.9% |
Yes | 258 | 34.1% | |
History of CKD | No | 472 | 62.4% |
Yes | 284 | 37.6% | |
Physical Exercises | Frequently | 444 | 58.7% |
Rarely | 312 | 41.3% | |
Financial Hardship | No | 424 | 56.1% |
Yes | 332 | 43.9% | |
Employment | Employed | 430 | 56.9% |
Retired | 260 | 34.4% | |
Unemployed | 66 | 8.7% |
Time | No. at Risk | No. of Diabetic kidney disease occurrences | Survival | Survival SE |
|---|---|---|---|---|
0 | 756 | 2 | 1.000 | 0.00000 |
3 | 682 | 8 | 0.987 | 0.00422 |
6 | 592 | 8 | 0.974 | 0.00609 |
9 | 494 | 22 | 0.934 | 0.01023 |
12 | 394 | 42 | 0.842 | 0.01638 |
15 | 300 | 42 | 0.734 | 0.02108 |
18 | 208 | 44 | 0.607 | 0.02468 |
21 | 96 | 76 | 0.329 | 0.02734 |
24 | 30 | 38 | 0.138 | 0.02349 |
27 | 6 | 4 | 0.111 | 0.02250 |
30 | 2 | 0 | 0.111 | 0.02250 |
Variable | Category | Events | Median Time | Mean Time (95% C.I.) | Test statistic | Log Rank’s P-Value |
|---|---|---|---|---|---|---|
Gender | Male | 144 | 19 | 18.37 | 4.4 | 0.04 |
Female | 142 | 20 | 19.64 | |||
Hypertension | No | 6 | NA | 28.65 | 54.6 | 1e-13 |
Yes | 280 | 19 | 18.02 | |||
Cardio-Vascular | No | 150 | 21 | 20.97 | 30.4 | 4e-08 |
Yes | 136 | 16 | 15.39 | |||
Level of Education | Primary | 109 | 18 | 16.78 | 39.8 | 2e-09 |
Secondary | 128 | 19 | 18.95 | |||
Tertiary | 49 | 22 | 22.19 | |||
Marital Status | Spouse | 206 | 20 | 21.08 | 20.3 | 7e-06 |
No Spouse | 80 | 19 | 17.81 | |||
Use of Tobacco | No | 56 | 24 | 23.64 | 111 | <2e-16 |
Yes | 230 | 16 | 16.39 | |||
Use of Alcohol | No | 78 | 22 | 22.33 | 76.9 | < 2e-16 |
Yes | 208 | 17 | 16.58 | |||
History of CKD | No | 18 | NA | 26.89 | 164 | <2e- 16 |
Yes | 268 | 16 | 16.32 | |||
Exercise | Frequently | 64 | 22 | 21.94 | 44 | 3e-11 |
Rarely | 222 | 18 | 17.34 | |||
Financial Hardship | No | 81 | 23 | 27.12 | 56.6 | 5e-14 |
Yes | 205 | 18 | 17.90 | |||
Employment | Employed | 56 | 23 | 22.12 | 35.2 | 2e-08 |
Retired | 174 | 20 | 18.84 | |||
Unemployed | 56 | 18 | 16.03 |
Factor | Unadjusted HR exp (coef) | Lower 95% | Upper 95% | P-value | |
|---|---|---|---|---|---|
Age | 1.019 | 1.007 | 1.031 | 0.00184 | |
Gender | Male | 1.275 | 1.011 | 1.608 | 0.0401 |
Hypertension | Yes | 10.9525 | 4.871 | 24.63 | 7.05e-09 |
CVD | Yes | 1.8830 | 1.493 | 2.375 | 9.2e-08 |
Weight | 1.0457 | 1.035 | 1.056 | <2e-16 | |
Education | Secondary | 0.6516 | 0.5024 | 0.845 | 0.00124 |
0.3515 | 0.2495 | 0.495 | 2.19e-09 | ||
Marital Status | Yes | 0.5618 | 0.4336 | 0.7279 | 1.28e-05 |
Tobacco | Yes | 4.225 | 3.152 | 5.665 | <2e-16 |
Alcohol | Yes | 3.002 | 2.312 | 3.897 | <2e-16 |
History of CKD | Yes | 11.675 | 7.235 | 18.84 | <2e-16 |
Exercise | Rarely | 2.471 | 1.867 | 3.269 | 2.42e-10 |
Financial Hardship | Yes | 9.935 | 4.686 | 21.06 | 2.12e-09 |
Employment | Retired | 1.845 | 1.361 | 2.502 | 7.97e-05 |
Unemployed | 2.994 | 2.062 | 4.347 | 8.24e-09 | |
DKD | Diabetic Kidney Disease |
CKD | Chronic Kidney Disease |
ESKD | End-Stage Kidney Disease |
DM | Diabetes Mellitus |
T2DM | Type 2 Diabetes Mellitus |
HTN | Hypertension |
CVD | Cardiovascular Disease |
eGFR | Estimated Glomerular Filtration Rate |
UACR | Urine Albumin-Creatinine Ratio |
HR | Hazard Ratio |
aHR | Adjusted Hazard Ratio |
CI | Confidence Interval |
SD | Standard Deviation |
AIC | Akaike Information Criterion |
C-index | Concordance Index |
| [1] | Thomas, M. C., Brownlee, M., Susztak, K., Sharma, K., Jandeleit-Dahm, K. A. M., Zoungas, S., Rossing, P., Groop, P.-H., & Cooper, M. E. (2015). Diabetic Kidney Disease. Nature Reviews. Disease Primers, 1(15018), 15018. |
| [2] | Jager, K. J., Kovesdy, C., Langham, R., Rosenberg, M., Jha, V., & Zoccali, C. (2019). A single number for advocacy and communication, worldwide, more than 850 million individuals have kidney diseases. Kidney International, 96(5), 1048-1050. |
| [3] | GBD 2021 Diabetes Collaborators. (2023). Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet, 402(10397). |
| [4] | Rhee, C. M., & Kovesdy, C. P. (2015). Spotlight on CKD deaths—increasing mortality worldwide. Nature Reviews Nephrology, 11(4), 199-200. |
| [5] | Mills, K. T., Xu, Y., Zhang, W., Bundy, J. D., Chen, C.-S., Kelly, T. N., Chen, J., & He, J. (2015). A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney International, 88(5), 950-957. |
| [6] | Abd ElHafeez, S., Bolignano, D., D’Arrigo, G., Dounousi, E., Tripepi, G., & Zoccali, C. (2018). Prevalence and burden of chronic kidney disease among the general population and high-risk groups in Africa: a systematic review. BMJ Open, 8(1), e015069. |
| [7] | Power, A., Duncan, N., & Goodlad, C. (2009). Advances and innovations in dialysis in the 21st century. Postgraduate Medical Journal, 85(1000), 102-107. |
| [8] | Tuttle, K. R., Bakris, G. L., Bilous, R. W., Chiang, J. L., de Boer, I. H., Goldstein-Fuchs, J., Hirsch, I. B., Kalantar-Zadeh, K., Narva, A. S., Navaneethan, S. D., Neumiller, J. J., Patel, U. D., Ratner, R. E., Whaley-Connell, A. T., & Molitch, M. E. (2014). Diabetic Kidney Disease: A Report From an ADA Consensus Conference. Diabetes Care, 37(10), 2864-2883. |
| [9] | Weldegiorgis, M., Smith, M., Herrington, W. G., Bankhead, C., & Woodward, M. (2019). Socioeconomic disadvantage and the risk of advanced chronic kidney disease: results from a cohort study with 1.4 million participants. Nephrology Dialysis Transplantation, 35(9), 1562-1570. |
| [10] | Cho, N. H., Shaw, J. E., Karuranga, S., Huang, Y., da Rocha Fernandes, J. D., Ohlrogge, A. W., & Malanda, B. (2018). IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Research and Clinical Practice, 138(1), 271-281. |
| [11] | Magliano, D., & Boyko, E. J. (2021). IDF Diabetes Atlas. International Diabetes Federation. |
| [12] | NCD Risk Factor Collaboration (NCD-RisC). (2016). Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4·4 million participants. The Lancet, 387(10027), 1513-1530. |
| [13] |
Mwaura, J. (2023, May 10). Diabetes Mellitus: Overview of Lab Diagnosis in Kenya. Labtestzote.com.
https://www.labtestzote.com/healthy-living/diabetes-mellitus-overview-of-lab-diagnosis-in-kenya/ |
| [14] | Wens, J., Vermeire, E., Van Royen, P., Sabbe, B., & Denekens, J. (2005). GPs’ perspectives of type 2 diabetes patients’ adherence to treatment: A qualitative analysis of barriers and solutions. BMC Family Practice, 6(1), 20. |
| [15] | Afkarian, M., Sachs, M. C., Kestenbaum, B., Hirsch, I. B., Tuttle, K. R., Himmelfarb, J., & de Boer, I. H. (2013). Kidney Disease and Increased Mortality Risk in Type 2 Diabetes. Journal of the American Society of Nephrology, 24(2), 302-308. |
| [16] | Parving, H.-H., Lewis, J. B., Ravid, M., Remuzzi, G., & Hunsicker, L. G. (2006). Prevalence and risk factors for microalbuminuria in a referred cohort of type II diabetic patients: A global perspective. Kidney International, 69(11), 2057-2063. |
| [17] | Phillips, K., Hazlehurst, J. M., Sheppard, C., Srikanth Bellary, Hanif, W., Muhammad Ali Karamat, Crowe, F. L., Stone, A., G. Neil Thomas, Javeria Peracha, Fenton, A., Sainsbury, C., Krishnarajah Nirantharakumar, & Dasgupta, I. (2023). Inequalities in the management of diabetic kidney disease in UK primary care: A cross‐sectional analysis of a large primary care database. Diabetic Medicine, 41(1). |
| [18] | Talie Fenta, E., Birhan Eshetu, H., Kebede, N., Ketema Bogale, E., Zewdie, A., Derbew Kassie, T., Fentabil Anagaw, T., Melaku Mazengia, E., & Shiferaw Gelaw, S. (2023). Prevalence and predictors of chronic kidney disease among type 2 diabetic patients worldwide, systematic review and meta-analysis. Diabetology & Metabolic Syndrome, 15(1). |
| [19] | Nakashima, A., Kato, K., Ohkido, I., & Yokoo, T. (2021). Role and Treatment of Insulin Resistance in Patients with Chronic Kidney Disease: A Review. Nutrients, 13(12), 4349. |
| [20] | Mu, X., Wu, A., Hu, H., Zhou, H., & Yang, M. (2023). Prediction of Diabetic Kidney Disease in Newly Diagnosed Type 2 Diabetes Mellitus. Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy, Volume 16, 2061-2075. |
| [21] | Shen, Y., Cai, R., Sun, J., Dong, X., Huang, R., Tian, S., & Wang, S. (2016). Diabetes mellitus as a risk factor for incident chronic kidney disease and end-stage renal disease in women compared with men: a systematic review and meta-analysis. Endocrine, 55(1), 66-76. |
| [22] | Parizadeh, D., Rahimian, N., Samaneh Akbarpour, Azizi, F., & Farzad Hadaegh. (2019). Sex-specific clinical outcomes of impaired glucose status: A long follow-up from the Tehran Lipid and Glucose Study. European Journal of Preventive Cardiology, 26(10), 1080-1091. |
| [23] | Shepard, B. D. (2019). Sex differences in diabetes and kidney disease: mechanisms and consequences. American Journal of Physiology-Renal Physiology, 317(2), F456-F462. |
| [24] | Hecking, M., Bieber, B. A., Ethier, J., Kautzky-Willer, A., Sunder-Plassmann, G., Säemann, M. D., Ramirez, S. P. B., Gillespie, B. W., Pisoni, R. L., Robinson, B. M., & Port, F. K. (2014). Sex-Specific Differences in Hemo`dialysis Prevalence and Practices and the Male-to-Female Mortality Rate: The Dialysis Outcomes and Practice Patterns Study (DOPPS). PLoS Medicine, 11(10), e1001750. |
| [25] | Tekalign, T., Guta, M. T., Awoke, N., Chichiabellu, T. Y., Meskele, M., Anteneh, G., Tura, T. S., & Workie, S. B. (2023). Time to Diabetic Nephropathy and its Predictors Among Diabetic Patients Treated in Wolaita and Dawuro Zone Hospitals, Ethiopia: A Retrospective Cohort Study. International Journal of Nephrology and Renovascular Disease, 16, 163-172. |
| [26] | Verma, A. (2016). Diabetic kidney disease and hypertension: A true love story. JOURNAL of CLINICAL and DIAGNOSTIC RESEARCH, 10(3). |
| [27] | Varleta, P., & Tagle, R. (2018). A feared combination: Hypertension and chronic kidney disease. The Journal of Clinical Hypertension, 21(1), 102-104. |
| [28] | Ke, C., S. Joseph Kim, Shah, B. R., Bierman, A. S., Lipscombe, L. L., Feig, D. S., & Booth, G. L. (2019). Impact of Socioeconomic Status on Incidence of End-Stage Renal Disease and Mortality After Dialysis in Adults With Diabetes. Canadian Journal of Diabetes, 43(7), 483-489. e4. |
| [29] | Saeed, M., Stene, L. C., Reisæter, A. V., Jenssen, T. G., Tell, G. S., Tapia, G., Joner, G., & Torild Skrivarhaug. (2022). End-stage renal disease: incidence and prediction by coronary heart disease, and educational level. Follow-up from diagnosis of childhood-onset type 1 diabetes throughout Norway 1973-2017. Annals of Epidemiology, 76, 181-187. |
| [30] | Cutler, D. M., & Lleras-Muney, A. (2010). Understanding differences in health behaviors by education. Journal of Health Economics, 29(1), 1-28. |
| [31] | Berkowitz, S. A., Meigs, J. B., DeWalt, D., Seligman, H. K., Barnard, L. S., Bright, O.-J. M., Schow, M., Atlas, S. J., & Wexler, D. J. (2015). Material Need Insecurities, Control of Diabetes Mellitus, and Use of Health Care Resources. JAMA Internal Medicine, 175(2), 257. |
| [32] | Walker, R. J., Garacci, E., Campbell, J. A., Harris, M., Mosley-Johnson, E., & Egede, L. E. (2020). Relationship Between Multiple Measures of Financial Hardship and Glycemic Control in Older Adults With Diabetes. Journal of Applied Gerontology, 40(2), 073346482091154. |
| [33] | Shen, Q., Jin, W., Ji, S., Chen, X., Zhao, X., & Behera, T. R. (2019). The association between socioeconomic status and prevalence of chronic kidney disease. Medicine, 98(11), e14822. |
| [34] | Kposowa, A. J., Aly Ezzat, D., & Breault, K. (2021). Diabetes Mellitus and Marital Status: Evidence from the National Longitudinal Mortality Study on the Effect of Marital Dissolution and the Death of a Spouse. International Journal of General Medicine, Volume 14, 1881-1888. |
| [35] | Sabanayagam, C., He, F., Nusinovici, S., Li, J., Lim, C., Tan, G., & Cheng, C. Y. (2023). Prediction of diabetic kidney disease risk using machine learning models: a population-based cohort study of Asian adults. ELife, 12, e81878. |
| [36] | Hu, C., & Steingrimsson, J. A. (2017). Personalized Risk Prediction in Clinical Oncology Research: Applications and Practical Issues Using Survival Trees and Random Forests. Journal of Biopharmaceutical Statistics, 28(2), 333-349. |
| [37] | Krishnamurthy, S., KS, K., Dovgan, E., Luštrek, M., Gradišek Piletič, B., Srinivasan, K., Li, Y.-C. (Jack), Gradišek, A., & Syed-Abdul, S. (2021). Machine Learning Prediction Models for Chronic Kidney Disease Using National Health Insurance Claim Data in Taiwan. Healthcare, 9(5), 546. |
| [38] | Usolo, S. W., Okoth, A., & Angwenyi, D. (2025). Modeling the effect of devolution on youth unemployment rates in Kenya using an autoregressive integrated moving average - intervention model. African Journal of Empirical Research, 6(3), 761-775. |
| [39] | Selby, N. M., & Taal, M. W. (2020). An updated overview of diabetic nephropathy: Diagnosis, prognosis, treatment goals, and latest guidelines. Diabetes, Obesity and Metabolism, 22(S1), 3-15. |
APA Style
Njoka, G. M., Muraya, M., Njoroge, E. W. (2026). Socio-economic, Demographic, and Clinical Predictors of Diabetic Kidney Disease Progression (Renal Function Decline) Among Adults with Diabetes: A Retrospective Cohort Study in Kenya. American Journal of Theoretical and Applied Statistics, 15(2), 27-39. https://doi.org/10.11648/j.ajtas.20261502.11
ACS Style
Njoka, G. M.; Muraya, M.; Njoroge, E. W. Socio-economic, Demographic, and Clinical Predictors of Diabetic Kidney Disease Progression (Renal Function Decline) Among Adults with Diabetes: A Retrospective Cohort Study in Kenya. Am. J. Theor. Appl. Stat. 2026, 15(2), 27-39. doi: 10.11648/j.ajtas.20261502.11
AMA Style
Njoka GM, Muraya M, Njoroge EW. Socio-economic, Demographic, and Clinical Predictors of Diabetic Kidney Disease Progression (Renal Function Decline) Among Adults with Diabetes: A Retrospective Cohort Study in Kenya. Am J Theor Appl Stat. 2026;15(2):27-39. doi: 10.11648/j.ajtas.20261502.11
@article{10.11648/j.ajtas.20261502.11,
author = {Grace Makena Njoka and Moses Muraya and Elizabeth Wambui Njoroge},
title = {Socio-economic, Demographic, and Clinical Predictors of Diabetic Kidney Disease Progression (Renal Function Decline) Among Adults with Diabetes: A Retrospective Cohort Study in Kenya},
journal = {American Journal of Theoretical and Applied Statistics},
volume = {15},
number = {2},
pages = {27-39},
doi = {10.11648/j.ajtas.20261502.11},
url = {https://doi.org/10.11648/j.ajtas.20261502.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajtas.20261502.11},
abstract = {Diabetic kidney disease (DKD) represents a major global health burden, yet predictive models often overlook socio-economic determinants that may independently influence disease progression. This retrospective cohort study aimed to identify socio-economic, demographic, and clinical predictors of diabetic kidney disease development among diabetic patients in Kenya and compare Cox regression with support vector machine (SVM) models for risk prediction. Data were collected from 756 adult diabetic patients attending Meru Teaching and Referral Hospital and Kerugoya Level 5 Hospital between January 2018 and July 2024 through medical record review and semi-structured questionnaires. Survival analysis employed Kaplan-Meier estimation, log-rank tests, multivariable Cox proportional hazards regression, and survival SVM modeling. During follow-up, 286 participants (37.8%) developed diabetic kidney disease. Multivariable Cox analysis identified seven significant predictors of diabetic kidney disease progression: older age at diabetes diagnosis (adjusted HR=1.023, p=0.002), male gender (HR=1.282, p=0.041), family history of chronic kidney disease (HR=6.919, pp=0.001), and financial hardship (HR=4.524, ppp=0.011) were protective. The SVM model demonstrated marginally superior predictive accuracy (C-index=0.775) versus Cox regression (C-index=0.770). These findings underscore that socio-economic factors function as independent risk modifiers beyond traditional clinical parameters, challenging conventional prediction paradigms that focus exclusively on biomedical indicators. The high incidence of diabetic kidney disease observed highlights an urgent public health challenge requiring integrated screening protocols that assess both clinical and socio-economic risk profiles at diabetes diagnosis. We recommend implementing targeted public health interventions that address financial barriers, promote educational attainment, and support employment opportunities for diabetic patients to mitigate diabetic kidney disease progression in resource-limited settings.},
year = {2026}
}
TY - JOUR T1 - Socio-economic, Demographic, and Clinical Predictors of Diabetic Kidney Disease Progression (Renal Function Decline) Among Adults with Diabetes: A Retrospective Cohort Study in Kenya AU - Grace Makena Njoka AU - Moses Muraya AU - Elizabeth Wambui Njoroge Y1 - 2026/03/05 PY - 2026 N1 - https://doi.org/10.11648/j.ajtas.20261502.11 DO - 10.11648/j.ajtas.20261502.11 T2 - American Journal of Theoretical and Applied Statistics JF - American Journal of Theoretical and Applied Statistics JO - American Journal of Theoretical and Applied Statistics SP - 27 EP - 39 PB - Science Publishing Group SN - 2326-9006 UR - https://doi.org/10.11648/j.ajtas.20261502.11 AB - Diabetic kidney disease (DKD) represents a major global health burden, yet predictive models often overlook socio-economic determinants that may independently influence disease progression. This retrospective cohort study aimed to identify socio-economic, demographic, and clinical predictors of diabetic kidney disease development among diabetic patients in Kenya and compare Cox regression with support vector machine (SVM) models for risk prediction. Data were collected from 756 adult diabetic patients attending Meru Teaching and Referral Hospital and Kerugoya Level 5 Hospital between January 2018 and July 2024 through medical record review and semi-structured questionnaires. Survival analysis employed Kaplan-Meier estimation, log-rank tests, multivariable Cox proportional hazards regression, and survival SVM modeling. During follow-up, 286 participants (37.8%) developed diabetic kidney disease. Multivariable Cox analysis identified seven significant predictors of diabetic kidney disease progression: older age at diabetes diagnosis (adjusted HR=1.023, p=0.002), male gender (HR=1.282, p=0.041), family history of chronic kidney disease (HR=6.919, pp=0.001), and financial hardship (HR=4.524, ppp=0.011) were protective. The SVM model demonstrated marginally superior predictive accuracy (C-index=0.775) versus Cox regression (C-index=0.770). These findings underscore that socio-economic factors function as independent risk modifiers beyond traditional clinical parameters, challenging conventional prediction paradigms that focus exclusively on biomedical indicators. The high incidence of diabetic kidney disease observed highlights an urgent public health challenge requiring integrated screening protocols that assess both clinical and socio-economic risk profiles at diabetes diagnosis. We recommend implementing targeted public health interventions that address financial barriers, promote educational attainment, and support employment opportunities for diabetic patients to mitigate diabetic kidney disease progression in resource-limited settings. VL - 15 IS - 2 ER -
Department of Physical Sciences, Chuka University, Chuka, Kenya
Department of Physical Sciences, Chuka University, Chuka, Kenya
Department of Physical Sciences, Chuka University, Chuka, Kenya
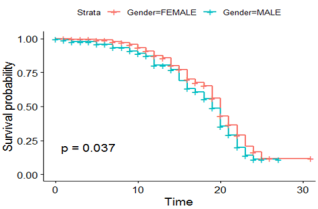
Figure 1. Kaplan Meier curves for Survival Probability Across Gender.
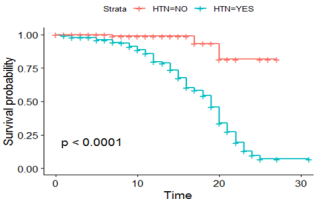
Figure 2. Kaplan Meier curves for Survival Probability Across Hypertension.
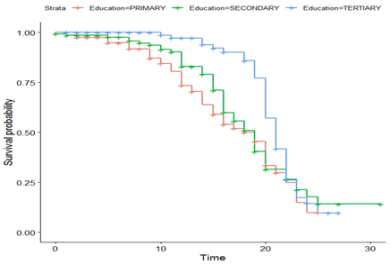
Figure 3. Kaplan Meier curves for Survival Probability Across Educational Levels.
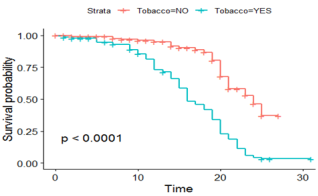
Figure 4. Kaplan Meier Curves for Survival Probability Across Tobacco Use.
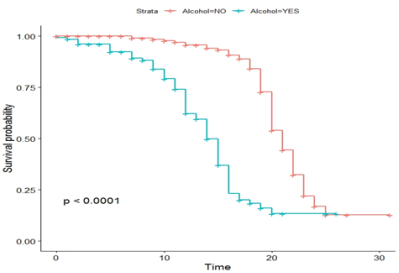
Figure 5. Kaplan Meier curves for Survival Probability Across Alcohol Use.
Information

