3. Results
3.1. Conceptual Framework
Economic theory provides a compelling rationale for introducing competitive structures within public agencies. The starting point is a well-established empirical regularity: organizations insulated from competitive pressure may systematically underperform. Leibenstein (1966) termed this X-inefficiency — the tendency of organizations shielded from external discipline to accumulate organizational slack, weaken effort norms, and managerial inertia without active cost minimization and output maximization.
| [8] | Leibenstein H. Allocative Efficiency vs. ‘X-Efficiency’. Am Econ Rev 1966; 56: 392–415. |
[8]
X-inefficiency arises from the absence of sufficient incentives to do better. The result, for public agencies, is that socially beneficial outputs — better health outcomes, faster drug approvals, more effective prevention programs — go unrealized because no competitive force compels efficient resource use. Recent cross-national evidence confirms that X-inefficiency in health systems remains substantial and measurable. A stochastic frontier meta-analysis found that health-care spending inefficiency—measured as the distance between a country’s health-adjusted life expectancy and the efficiency frontier — persisted in most countries during 1995-2022.
| [10] | Lastuka A, Breshock MR, Hay SI, et al. Global, regional, and national health-care inefficiency and associated factors in 201 countries, 1995-2022: a stochastic frontier meta-analysis for the Global Burden of Disease Study 2023. Lancet Glob Health 2025; 13: e1349–e1357.
https://doi.org/10.1016/S2214-109X(25)00178-0 |
[10]
In particular, the study found that governance improvements were among the strongest predictors of efficiency gains, suggesting that structural reforms may be promising.
The intuition from industrial organization economics reinforces this diagnosis. Under monopoly conditions, a single seller restricts output below the socially optimal level to maintain pricing power, generating deadweight loss — the welfare foregone when market power prevents transactions that would otherwise occur.
| [11] | Harberger A. Monopoly and Resource Allocation. 1954; 44: 77–87. |
[11]
Monopsony presents the mirror-image problem: a single buyer suppresses the quantity it purchases, driving the prices it pays to suppliers below the competitive equilibrium and exploiting workers and vendors alike.
| [12] | Blair R, Harrison J. Antitrust Policy and Monopsony. Cornell Law Rev 1991; 76: 297–340. |
[12]
In both cases, the absence of a competitive counterpart allows the dominant party to capture surplus at the expense of overall welfare. Transitioning from a monopoly or monopsony to a duopoly or duopsony introduces a second actor, exerting competitive pressure that moves output and prices toward socially optimal levels and recovers a portion of the deadweight loss.
| [13] | Carson R. The Welfare Loss from Monopoly Re-visited: Rent Seeking and Protectionism. Int J Bus Econ Res 2021; 10: 141–146. https://doi.org/10.11648/j.ijber.20211004.14 |
| [14] | Tirole J. The Theory of Industrial Organization. MIT Press, 1988. |
[13, 14]
.
Public agencies do not restrict output (or quantity purchased) to extract surplus, so the monopoly (or monopsony) analogy does not apply directly. Its value is structural and intuitive: it illustrates why the absence of a competitive counterpart tends to produce inefficiency, and why introducing one exerts discipline. The underlying mechanism in the public-sector context is not price competition but comparative accountability — and for this, a different theoretical tool is required.
Shleifer (1985) proposed yardstick competition as precisely such a tool for settings where direct market competition is absent.
Rather than relying on price signals, a regulator benchmarks the performance of one entity against comparable entities, infers an efficiency frontier from the comparison, and uses that information to set cost targets and allocate resources. The mechanism requires no market: it requires only that two or more comparable units exist and that their performance can be measured and compared. Competitive pressure is thereby replicated through comparative evaluation rather than through consumer choice or price rivalry. For example, this mechanism has been operationalized in the U.S. Medicare Hospital Value-Based Purchasing (VBP) Program, which annually redistributes billions of dollars based on hospitals’ relative quality performance. It has been demonstrated that yardstick incentives in the VBP program were associated with quality improvement, suggesting comparative accountability can function as intended within complex public health delivery systems.
| [15] | Lim JM, Moon K, Savin S. Searching for the Best Yardstick: Cost of Quality Improvements in the U.S. Hospital Industry. Manag Sci 2024; 70: 3769–3788.
https://doi.org/10.1287/mnsc.2023.4875 |
[15]
.
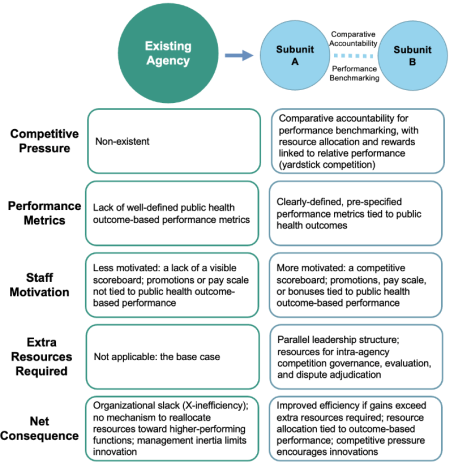
Figure 1. Intra-Agency Competition Framework.
Together, X-inefficiency theory and yardstick competition establish the theoretical foundation for the intra-agency competition framework proposed here. X-inefficiency identifies the source of welfare loss in insulated public agencies; yardstick competition provides the governance mechanism for recovering it. The monopoly-to-duopoly (or monopsony-to-duopsony) transition serves as a useful structural analogy — illustrating why a second actor changes incentives — but the operative logic is benchmarking rather than market rivalry.
Specifically, the proposed intra-agency competition framework involves splitting a single agency into two autonomous, competing subunits that perform the same function and are responsible for delivering the same mandate (
Figure 1). Rather than relying on top-down, discretionary budget reductions — which are susceptible to political influence and do not inherently reward efficiency — this structure activates what
Figure 1 identifies as the framework's key mechanism: comparative accountability for performance benchmarking, with resource allocation and rewards linked to relative performance outcomes. This governance logic is consistent with yardstick competition theory. On the existing agency side,
Figure 1 illustrates the baseline conditions this mechanism is designed to remedy: a lack of competitive pressure, vaguely defined performance metrics, staff motivation weakened by the absence of a visible scoreboard, and, as a result, organizational slack (X-inefficiency) with no internal mechanism to reallocate resources toward higher-performing functions. Under the intra-agency competition framework, each subunit would face incentives to minimize costs, improve service quality, and innovate, because superior performance could be rewarded with resources, institutional recognition, or expansion, while underperformance would carry real consequences. By embedding these competitive incentives within the institutional architecture of a public agency, the framework may channel self-interest toward socially desirable outcomes without requiring continuous external oversight or politically contested spending decisions. Nonetheless, as
Figure 1 makes explicit, this net benefit is conditional on efficiency gains exceeding the extra resources required to sustain the parallel governance structure. In this context, competition does not replace the public interest as the governing objective — it is intended to operationalize and optimize it.
This approach is theoretically attractive precisely because it does not depend on the accuracy or biases of any single decision-maker or a group of decision-makers' judgment. Instead, it harnesses decentralized information and competitive dynamics to surface efficiencies that centralized, discretionary processes are unlikely to identify. The result is a governance structure that is both more adaptive, more accountable, and more efficient than the monopolistic (or monopsonist) status quo.
3.2. Potential Applications in the U.S.
The intra-agency competition framework can be applied across a range of public health functions, including direct service delivery, regulatory oversight, and public health practice. Rather than being limited to a single agency type, the framework is sufficiently flexible to accommodate the diverse organizational structures and mandates found throughout the public health system.
3.2.1. Service Delivery
The most extensively studied case is the NHS internal market, introduced in England in the 1990s under the Conservative government and continued in a modified form under New Labour into the 2000s. This model structurally separated purchasers from providers within a single-payer system and promoted patient choice among competing providers as a mechanism to drive quality and value.
The purchaser-provider split created incentives for hospitals and other providers to attract patients by improving services and controlling costs, effectively embedding market-like dynamics within a publicly funded framework. Evidence suggests that the NHS internal market led to lower costs and increased provider efficiency over time, although quality declined initially during the 1990s before improving in the 2000s as the model matured, performance metrics were refined, and accountability mechanisms were strengthened.
Specifically, Propper, Burgess, and Gossage (2008) found that during the 1990s price competition phase, hospitals in more competitive markets reduced waiting times but experienced modestly higher acute myocardial infarction (AMI) death rates—a result attributed to hospitals optimizing on measured dimensions (waiting times) while neglecting unmeasured ones (clinical mortality).
In contrast, following the post-2006 reforms that introduced fixed-price competition and expanded patient choice, Cooper et al. (2011) found that patients in high-competition areas experienced measurably lower post-reform AMI mortality than those in low-competition areas, providing causal evidence that competition with well-designed, fixed-price metrics can improve clinical outcomes in a publicly funded health system.
.
One potential application of this framework to the U.S. would be the Office of Medicare Management within the CMS, which administers the traditional FFS Medicare program. This office could be divided into two autonomous subunits, each charged with improving health outcomes for FFS beneficiaries and managing costs more effectively, but operating independently and being evaluated against one another. To implement this, in an initial phase, the two subunits could be assigned responsibility for distinct geographic regions, competing on the basis of risk-adjusted, pre-specified performance metrics such as per-beneficiary spending, preventable hospitalization rates, and chronic disease management outcomes. This geographic separation would allow operational differences to emerge and be measured without direct overlap. As the program matures and administrative capacity develops, the subunits could then expand into the same geographic areas, competing directly for FFS beneficiary enrollment and driving further gains in quality and efficiency. The number of competing subunits need not be limited to two; introducing additional subunits could generate further competitive pressure and yield greater efficiency gains, consistent with economic theory suggesting that welfare improvements increase as markets move away from duopoly toward more competitive structures. See more implementation details in Section 3.4.
Unlike the UK’s NHS, U.S. health plans and providers are often privately owned and thus not government agencies. There are no close examples of competing public agencies within the U.S. healthcare system; below, we discuss some programs that introduce competition by government purchasers to illustrate possible outcomes in the U.S context.
The Medicare Advantage program, in which private health plans compete with one another, may not be a close example, but it exhibits competitive features. However, largely because it has a higher cost benchmark than traditional Medicare, it remains unclear whether Medicare Advantage saves money.
.
In contrast, Medicare's Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) competitive bidding program offers a compelling domestic success story. Launched by CMS, the program replaced administratively set fee schedules with a competitive bidding process in which suppliers submit bids to provide covered equipment and supplies, with contracts awarded to those offering the best combination of price and quality. This market-based mechanism reduced Medicare spending on durable medical equipment by 47% during the five years following the program's launch,
| [20] | Ding H, Duggan M, Starc A. Getting the Price Right? The Impact of Competitive Bidding in the Medicare Program. Rev Econ Stat 2025; 107: 204–220.
https://doi.org/10.1162/rest_a_01249 |
[20]
representing substantial savings for both the program and beneficiaries. Importantly, these cost reductions were achieved without compromising access to necessary equipment or increasing adverse patient outcomes, addressing the concern that competitive mechanisms in healthcare inevitably trade cost savings for quality.
.
At the state level, a number of states have employed competitive bidding to procure managed care health plan services for their Medicaid and Children's Health Insurance Program (CHIP) beneficiaries for more than a decade.
Under these arrangements, health plans submit bids to serve enrollees within defined geographic regions, with contracts awarded based on price, quality metrics, and network adequacy. While this approach has demonstrated meaningful cost reductions, the evidence base remains limited. No rigorous, peer-reviewed studies have been published evaluating these programs, and the available descriptive analyses suggest a concerning trade-off: although competitive procurement reduced expenditures, it also introduced quality problems in some instances, including disruptions to continuity of care and to beneficiaries' access to established providers.
| [25] | Paringer L, McCall N. How Competitive Is Competitive Bidding? Health Aff (Millwood) 1991; 10: 220–230.
https://doi.org/10.1377/hlthaff.10.4.220 |
| [26] | Dyckman Z. Competitive Bidding for Health Care Services. U.S. Department of Health and Human Services, Health Care Financing Administration, Office of Research and Demonstrations, 1986. |
[25, 26]
These findings underscore the importance of robust performance standards and oversight mechanisms when introducing competitive frameworks into publicly administered health programs.
3.2.2. Regulatory Oversight
Internal competition need not be confined to service delivery agencies — it could also be applied productively within regulatory bodies. Consider the CDER within the FDA, which evaluates and approves new pharmaceutical products. Concerns have been raised that CDER is being overly cautious, potentially delaying patient access to new therapies relative to European counterparts — a phenomenon sometimes described as “drug lag.”
| [27] | Carpenter D. Reputation and Power: Organizational Image and Pharmaceutical Regulation at the FDA. Princeton University Press, 2014. |
[27]
.
Dividing CDER into two or more competing subunits could introduce a self-correcting dynamic into the regulatory process. In an initial phase, subunits might overcompensate in an effort to attract new drug applications from sponsors — potentially erring toward leniency. However, this is precisely where well-designed performance metrics become essential. By evaluating subunits on a scorecard of outcomes (see Section 3.2.4 Performance Measurement), the competitive framework would create incentives for accuracy and thoroughness rather than for speed alone.
Over time, competition encourages an iterative adjustment process in which subunits improve their approaches, converging toward a more optimal balance between safety and efficacy. Rather than replacing regulatory judgment, this framework sharpens it by subjecting each subunit's decision-making to comparative scrutiny and accountability.
3.2.3. Public Health Practice
Even a public health agency such as the CDC can leverage internal competition to improve outcomes. Consider the NCCDPHP, which oversees programs addressing the leading causes of death and disability in the U.S., including cardiovascular disease, diabetes, obesity, and cancer. The country could be divided into multiple geographic regions, with the NCCDPHP organized into a corresponding number of autonomous subunits, each responsible for managing chronic disease prevention and health promotion activities within its assigned region. Subunits would compete with each other and be evaluated against one another on risk-adjusted, region-specific performance metrics, creating incentives for each to identify and adopt the most effective programmatic approaches.
A structurally similar model has already been adopted by the Environmental Protection Agency (EPA), which divides the country into ten geographic regions, benchmarks outcomes across them, and implicitly links performance to funding allocations.
This regional structure creates a form of comparative accountability that shares certain features with the intra-agency competition framework proposed here. However, the EPA model falls short in one important respect: it does not incorporate operating costs into its performance evaluation, leaving efficiency incentives incomplete. A more fully realized intra-agency competition framework would integrate both outcome quality and cost-effectiveness into the performance metrics used to evaluate and differentiate subunits.
3.2.4. Performance Measurement
Subunit performance metrics must be carefully designed to reflect both outcomes and operating costs, remain aligned with each agency's statutory mandates, and consistently serve the public interest. The appropriate metrics will vary across agencies, depending on the nature of their functions and the extent to which their outputs can be quantified in financial terms.
For the FFS Medicare program, which provides insurance services already available in the private market, performance metrics can be drawn directly from analogous private-sector benchmarks. Suitable measures would include total surplus — defined as the sum of Part A budget and Part B premiums minus claims paid and subunit operating costs — as well as return on investment (ROI), risk-adjusted health outcomes, and beneficiary satisfaction. A composite measure may be considered, such as an ROI weighted by health outcomes (see Section 3.4 for an example). These metrics would allow subunits to be evaluated on both fiscal stewardship and the quality of care delivered to enrollees, creating balanced incentives that discourage cost-cutting at the expense of outcomes.
For the CDER, the challenge is more complex, given the inherent difficulty of monetizing drug safety and efficacy. In this context, QALYs — a widely used health economic measure that integrates both length and quality of life — provide a rigorous and internationally recognized outcome metric. Subunit performance could be evaluated on total QALYs gained through approved therapies, as well as cost-effectiveness, defined as the ratio of QALYs gained to subunit operating costs. This framework rewards subunits that efficiently approve effective, high-value therapies, while penalizing those that incur high costs relative to health gains.
Similar metrics could be adapted for the NCCDPHP, where the relevant outcomes include reductions in chronic disease burden, preventable hospitalizations, and premature mortality — all of which can be expressed in QALY terms — alongside a corresponding measure of cost-effectiveness. Across all agencies, the overarching principle is that performance metrics should include both outcome and cost dimensions, be resistant to gaming, and be directly tied to each agency's public health mandate.
3.2.5. Financial Incentives
A fundamental challenge in applying competitive frameworks within federal government agencies is the absence of residual claimants
— that is, unlike private sector firms, where shareholders capture the financial gains from efficiency improvements, no individual or group within a public agency has a direct financial stake in the surplus generated by better performance. This structural feature weakens the natural incentive for efficiency that competition ordinarily produces in markets, and must be deliberately addressed through the design of meaningful monetary incentives.
Within the constraints of federal employment law and civil service regulations, several mechanisms are available.
For frontline staff and mid-level personnel, performance-based rewards, quality-step increases, and group-oriented productivity incentives can be deployed to align individual behavior with subunit goals. For leadership roles within competing subunits, Senior Executive Service performance bonuses represent an important lever, as they allow agencies to differentiate compensation based on measurable outcomes rather than tenure alone.
Careful design of these incentive structures is essential.
Incentives that are too narrowly focused on short-term metrics can discourage investment in long-term capacity building, while individually oriented rewards may undermine the collaborative behavior necessary for effective public health delivery. Conversely, incentives that are too diffuse or disconnected from measurable performance may fail to motivate meaningful change. The goal is a balanced incentive architecture that rewards both individual contribution and collective subunit performance, sustains focus on long-term performance, and remains consistent with the federal government's broader obligations of equity, transparency, and accountability.
3.3. Potential Applications in Other Countries
The intra-agency competition framework described above is not limited to the U.S. In any country with a functioning rule of law, independent regulatory institutions, and transparent performance accountability, the same structural logic applies. This includes most of Western Europe, Canada, Australia, and Japan — jurisdictions that share the institutional prerequisites necessary for competitive incentives to operate as intended rather than being distorted by political interference or regulatory capture. That said, even within these settings, implementation would need to be carefully tailored to each country's political economy, existing bureaucratic structures, and the preferences of key institutional stakeholders.
The most direct application is to countries with publicly funded healthcare delivery systems, such as Brazil and Canada. Where governments act as the dominant purchaser of health services — a monopsonistic position analogous to Medicare in the U.S. context — splitting delivery responsibilities across two or more autonomous, competing provider entities could generate efficiency gains and innovation incentives similar to those described above. The UK's NHS offers the most extensively studied precedent. Countries such as Canada, France, Germany, Australia, and Brazil, which similarly combine public financing with a mix of public and private delivery, may find analogous structures worth exploring within their existing institutional architectures.
The framework may also be relevant to regulatory agencies. Bodies such as the European Medicines Agency, which performs functions comparable to the U.S. FDA, operate in environments where performance benchmarking, structured peer review, or competitive allocation of review responsibilities could reduce bottlenecks and improve decision quality.
Public health agencies analogous to the U.S. CDC — including the UK Health Security Agency, the European Centre for Disease Prevention and Control, and the Public Health Agency of Canada — similarly operate in environments where competitive accountability mechanisms could strengthen performance, though the same implementation considerations apply.
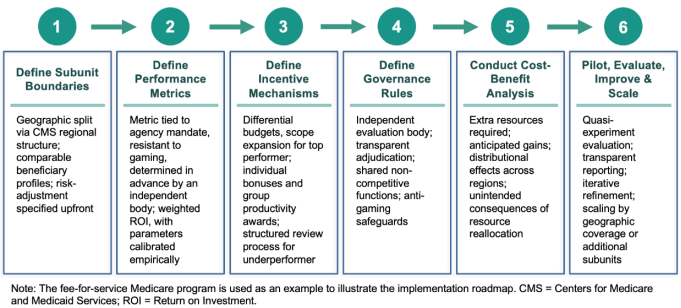
3.4. Potential Implementation Roadmap
The following roadmap illustrates one possible approach to implementation, serves as a potential working model, and is not intended to be prescriptive or exhaustive. The FFS Medicare program is used as a running example throughout; it is chosen because it represents the most operationally mature and institutionally well-understood context for applying the framework in the U.S. The specific sequencing, design choices, and governance arrangements described below will require adaptation to specific contexts and to evolving legal and political conditions.
Figure 2. Potential Implementation Roadmap.
Step (1): Define subunit boundaries. The first step is to determine how the agency will be divided into competing subunits. In the case of FFS Medicare, a geographic split is the most operationally feasible initial design, considering the existing 10 CMS regional offices. To the extent possible, geographic assignment should be designed to ensure comparability in baseline beneficiary health status and existing provider capacity. In addition, risk-adjustment procedures should be specified in advance so that performance differences can be attributed to subunit-level management and innovation.
Step (2): Define performance metrics. Performance metrics must be specified before the pilot begins, tied directly to each agency’s public mandate, and resistant to gaming. For the FFS Medicare pilot, a candidate composite metric may be a beneficiary-satisfaction-weighted ROI, as defined below, with λ empirically calibrated to ensure subunit operating costs are on comparable scales. It is intended to incentivize subunits to improve the value of care delivered to beneficiaries, reduce claims paid, and remain mindful of beneficiary satisfaction and subunit operating costs. This is just one possibility, and we acknowledge that defining a composite metric warrants further research. Nevertheless, the metric, its components, and the calibration parameters should be set in advance by an independent body and should not be modifiable by either competing subunit.
Weighted ROI =[(Expected spending per beneficiary − Actual spending per beneficiary − λ × Subunit operating costs per beneficiary) / (Actual spending per beneficiary + λ × Subunit operating costs per beneficiary)]× Risk-adjusted beneficiary satisfaction weight
Step (3): Define resource reallocation and incentive mechanisms. Competitive incentives require that superior performance be rewarded with tangible consequences. For the FFS Medicare pilot, resource reallocation might take several forms: (a) differential budget allocations in subsequent fiscal years, weighted toward the subunit achieving better performance; (b) expansion of operational scope or geographic responsibility for higher-performing subunits; and (c) personnel incentives, including Senior Executive Service performance bonuses for leadership and group productivity awards for staff. Incentive design should balance individual and collective rewards to avoid undermining collaborative behavior, and should be shielded from political interference to maintain credibility. Importantly, underperformance should trigger a structured review process — conducted by the independent governance body — rather than automatic downsizing or workforce reductions. This is essential for political feasibility: it signals to federal employees, unions, and agency leadership that the framework is designed to improve performance through accountability and learning, not to serve as a mechanism for arbitrary budget cuts, which the framework is explicitly proposed as an alternative to.
Step (4): Define governance rules. Clear governance rules are essential to ensure competition drives performance improvement rather than internal lobbying or bureaucratic rivalry. For the FFS Medicare pilot, governance rules should specify: (a) who controls the performance evaluation process—ideally an independent body without interference from either subunit or shared political leadership; (b) how disputes over metric interpretation or performance assessment will be adjudicated; and (c) what safeguards will prevent gaming, including regular metric review, whistleblower protections, and penalties for misreporting. Shared functions requiring coordination—such as beneficiary data infrastructure and fraud detection—should be explicitly designated as non-competitive and managed through joint governance mechanisms.
Step (5): Conduct a pre-pilot cost-benefit analysis. Before implementing the pilot, a rigorous cost-benefit analysis should be conducted to assess whether the anticipated efficiency gains are likely to outweigh the additional resources required relative to the status quo. For the FFS Medicare example, cost inputs would include the administrative overhead of maintaining two parallel management structures, designing and operationalizing performance metrics, establishing independent evaluation capacity, and adjudicating performance disputes. The cost-benefit analysis should distinguish upfront costs from maintenance costs. Benefits may include projected savings to Medicare (= expected spending − actual spending) under intra-agency competition. It should also explicitly model distributional effects, including the risk that efficiency gains may be unevenly distributed across geographies or beneficiary populations, as well as the consequences of following resource reallocation.
Step (6): Pilot, evaluate, improve, and scale. Ideally, the pilot should be implemented as a quasi-experimental evaluation. For the FFS Medicare pilot, appropriate comparison groups might include matched geographic regions not subject to the intervention with historically comparable baseline periods. Based on results, the framework design—including metric weights, incentive structures, and governance rules—should be iteratively refined before any decision to scale. If the pilot demonstrates net positive welfare effects—improved performance metrics relative to controls, acceptable unintended consequences, and a favorable cost-benefit ratio—the framework may be expanded in two ways: (a) expanding geographic coverage so that the two FFS Medicare subunits operate in overlapping rather than distinct regions, introducing direct enrollment competition; and (b) introducing additional competing subunits to further welfare gains. Scaling decisions should be evidence-based because the framework's theoretical efficiency gains are not guaranteed but conditional on the specific design choices made in Steps 1 through 5.
4. Discussion
The intra-agency competition framework proposed here may offer a principled mechanism for improving efficiency and population health outcomes within the U.S. federal public health agencies and those in other countries. Unlike discretionary budget cuts, which may reduce capacity in ways that are difficult to target or reverse, competition-based reforms tie resource allocation directly to performance, creating continuous pressure to improve outputs relative to costs. This approach is consistent with the broader tradition of NPM reforms and with economic theory suggesting that moving from a monopoly to a duopoly structure generates welfare gains by reducing deadweight loss.
We acknowledge that, to our knowledge, no government has formally implemented intra-agency competition in the precise form proposed here—that is, the deliberate division of a single public agency into two autonomous, competing subunits evaluated against one another on performance metrics. The examples in the healthcare field reviewed in this paper—the NHS internal market, the DMEPOS competitive bidding program, and Medicaid managed care procurement—involve competition among legally distinct service or product providers rather than within a single agency. The governance challenges, incentive dynamics, and unintended consequences of true intra-agency competition may differ in important ways from those documented in the analogous literature. The U.S. EPA is another example, but competition among regional offices is implicit and is not tied to operating costs. Filling this knowledge gap requires empirical research that does not yet exist. By articulating a theoretical framework, this paper provides the conceptual infrastructure necessary to design and evaluate pilots capable of generating the evidence.
There are meaningful implementation barriers that warrant careful consideration. One significant challenge lies in performance monitoring. Measuring subunit operating costs is relatively straightforward, but assessing the outcomes that public agencies are ultimately designed to produce is considerably more complex. Relevant metrics would include risk-adjusted health outcomes, QALYs, and program beneficiary satisfaction — each of which requires methodological rigor and sustained investment to produce reliably. Sound, mature methodologies for measuring these outcomes have been developed in the health economics literature, and tools such as the EQ-5D, SF-6D, and HUI3 instruments are already widely used in clinical and policy contexts.
| [31] | Pickard AS, Law EH, Jiang R, et al. United States Valuation of EQ-5D-5L Health States Using an International Protocol. Value Health 2019; 22: 931–941.
https://doi.org/10.1016/j.jval.2019.02.009 |
| [32] | Feeny D, Furlong W, Torrance GW, et al. Multiattribute and Single-Attribute Utility Functions for the Health Utilities Index Mark 3 System. Med Care 2002; 40: 113. |
| [33] | Brazier J, Roberts J, Deverill M. The estimation of a preference-based measure of health from the SF-36. J Health Econ 2002; 21: 271–292.
https://doi.org/10.1016/S0167-6296(01)00130-8 |
[31-33]
However, applying them systematically at the population level — for example, to evaluate the comparative performance of competing FDA or CDC subunits — would require dedicated data infrastructure, independent evaluation capacity, and ongoing resource commitments. These challenges are not unique to the United States; any country adopting this framework would face comparable demands on its measurement and evaluation systems.
Another barrier is legal, though in the U.S., this may be less significant than it first appears. New legislation may not be required, given that the executive branch has broad authority to reorganize administrative agencies. In
Trump v. American Federation of Government Employees (2025), the U.S. Supreme Court stayed a lower court injunction blocking large-scale agency reductions in force and reorganizations, finding that the executive order directing those actions was likely lawful — signaling that the current Court leans toward broad executive discretion in this domain.
The case has not been finally resolved on the merits. A loss for the Trump administration would indicate that Congressional authorization is required. Furthermore, the financial incentive mechanisms required to make this framework operational — such as performance-based budget allocation and differential resource distribution between subunits — are grounded in existing administrative and appropriations law, and would likely not require new statutory authority regardless of how the reorganization question is ultimately resolved.
In other countries, the legal picture is more varied. In the United Kingdom, structural reorganization of public agencies has historically required primary legislation, as illustrated by the National Health Service and Community Care Act 1990,
which established the NHS internal market, and the Health and Social Care Act 2012,
which restructured NHS governance. Parliamentary systems in Canada, Australia, and most European countries similarly vest reorganization authority primarily in the legislature rather than the executive, meaning that implementing this framework would likely require either new enabling legislation or amendment of existing agency mandates. In more centralized systems, the executive retains somewhat broader administrative discretion, which could ease implementation — though parliamentary or constitutional constraints would still apply in specific contexts.
Beyond legal and institutional constraints, political feasibility is a critical determinant of whether intra-agency competition can be implemented in practice. Several political actors may serve as facilitators. In the U.S., for example, fiscal conservatives in Congress and among the electorate who prioritize deficit reduction and government efficiency represent a natural constituency for performance-based reforms that offer an evidence-grounded alternative to arbitrary spending cuts. Budget oversight bodies—including the Congressional Budget Office and the Government Accountability Office—may also support the framework if rigorous cost-benefit projections are credible and independently validated. Conversely, several actors are likely to resist implementation. Federal employee unions have historically opposed reforms that introduce competitive pressures on workforce structure, compensation, and job security.
Existing agency leadership may resist the institutional fragmentation and loss of unified authority that splitting agencies would entail. Congressional appropriators with close relationships to specific agencies may also oppose restructuring that disrupts established funding channels. Feasible implementation strategies to navigate these political dynamics include: framing the framework as an alternative to arbitrary cuts rather than a complement to them, which may broaden its political coalition; engaging federal union leadership early in framework design to address workforce concerns and incorporate labor protections into governance rules; initiating reform through voluntary pilot programs in lower-profile agency contexts before seeking broader legislative authorization; and building an independent evidence base through transparent pilot evaluations that can withstand adversarial political scrutiny.
Furthermore, the rules of competition must be carefully designed to preempt unintended consequences. Subunits within the same agency will compete for budgets, talent, and institutional recognition — but they also share a parent agency, congressional appropriators, and political leadership. This creates a real risk that competition devolves into internal lobbying and bureaucratic turf wars rather than genuine performance improvement. This risk is well recognized in the public administration literature.
Safeguards should therefore include independent performance evaluation, transparent metric design, and clear adjudication rules to ensure that competitive incentives reward outcomes rather than political maneuvering.
Finally, it is worth noting that the intra-agency competition framework proposed in this paper complements rather than replaces other efficiency-promoting strategies, including process improvement, technology adoption, and workforce development. Its distinctive contribution lies in creating structural incentives for ongoing improvement, rather than relying on episodic management interventions. Future research should evaluate the welfare effects of specific pilot implementations, examine the optimal design of performance metrics for different agency types, and investigate how intra-agency competition interacts with existing civil service regulations, collective bargaining agreements, and statutory mandates. As federal agencies face mounting pressure to demonstrate fiscal responsibility while maintaining and improving population health outcomes, evidence-based frameworks such as this one will be essential for informing reform efforts.
Nevertheless, the framework has important limitations that must be addressed in institutional design. First, competition often exacerbates inequality. If CDER subunits are evaluated on QALY-based metrics, there is a risk that drugs targeting rare diseases—which typically yield smaller aggregate QALY gains—would be deprioritized. Rare disease programs should therefore be explicitly excluded from intra-agency competition, with dedicated funding and evaluation mechanisms.
Second, competition may hinder collaboration between subunits, leading to fragmentation in regulatory actions or service delivery, duplication of effort, and gaps in programs that require coordinated national responses, such as infectious disease surveillance and emergency preparedness. Institutional safeguards—including shared data infrastructure, joint planning processes, and coordination mandates—would be required to mitigate this risk.
Third, the costs of establishing and operating a competitive framework—including the overhead of maintaining two parallel administrative structures, designing and monitoring performance metrics, and adjudicating disputes—may offset efficiency gains, at least in the short term. A rigorous upfront cost-benefit analysis is therefore essential before implementation. Pilot programs in well-defined, lower-risk contexts would provide valuable evidence on feasibility, unintended consequences, and net welfare effects before any large-scale rollout.