Abstract
Background: Osteoporosis and osteopenia represent major yet underrecognized public health challenges in low- and middle-income countries. In South Asia, demographic aging, nutritional inadequacies, sedentary lifestyles, and limited access to diagnostic facilities have contributed to a rising burden of bone mineral disorders. Bangladesh, in particular, lacks large comparative studies evaluating bone health across gender and residential settings. Aim: The present study aimed to determine the prevalence of osteopenia and osteoporosis among adults in Bangladesh and to examine the influence of gender, age, and residential setting (urban versus rural) on bone mineral density. Methods: A cross-sectional analytical study was conducted among 380 adults equally sampled from urban Dhaka and rural Sylhet. Bone mineral density was evaluated using WHO-defined T-score and Z-score criteria. Statistical analyses included descriptive statistics, chi-square tests, independent t-tests, Pearson correlation analysis, and multivariable logistic regression to identify independent predictors of abnormal bone health. Results: Abnormal bone mineral density was detected in 80.5% of participants, with osteopenia constituting the majority (72.6%). Females exhibited significantly lower mean T-scores and higher prevalence of osteoporosis compared to males. Age showed a strong inverse correlation with both T-score and Z-score. Gender and age emerged as independent predictors, while residential region showed no significant association. Conclusion: The study highlights a substantial burden of subclinical and clinical bone disease in Bangladesh, particularly among women and older adults. These findings emphasize the need for early screening, preventive interventions, and national osteoporosis control strategies.
Keywords
Osteoporosis, Osteopenia, Bone Mineral Density, Gender Disparity, Aging, Bangladesh
1. Introduction
Osteoporosis is a chronic, progressive skeletal disorder characterized by diminished bone strength, resulting from reductions in bone mass and deterioration of bone microarchitecture
. It is a major contributor to fragility fractures, which are associated with significant morbidity, disability, and increased mortality, particularly among older adults
| [2] | World Health Organization. (1994). Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Report of a WHO Study Group. World Health Organization. |
[2]
. Globally, osteoporosis affects more than 200 million individuals and accounts for approximately 8.9 million fractures annually, placing a substantial burden on healthcare systems worldwide
| [3] | Johnell, O., & Kanis, J. A. (2006). An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis International, 17(12), 1726–1733.
https://doi.org/10.1007/s00198-006-0172-4 |
[3]
.
While osteoporosis has traditionally been perceived as a disease of affluent nations, recent evidence indicates a rapid rise in its prevalence in low- and middle-income countries
. Factors such as nutritional deficiencies, low dietary calcium intake, vitamin D insufficiency, early menopause, physical inactivity, and increasing life expectancy contribute significantly to this trend
. In South Asia, these risk factors are compounded by socioeconomic disparities and limited public health infrastructure, leading to delayed diagnosis and under-treatment
| [6] | NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. (2001). Osteoporosis prevention, diagnosis, and therapy. JAMA, 285(6), 785–795.
https://doi.org/10.1001/jama.285.6.785 |
[6]
.
Gender plays a pivotal role in osteoporosis epidemiology. Women experience accelerated bone loss following menopause due to estrogen deficiency, resulting in a markedly higher lifetime fracture risk compared to men
. Postmenopausal women may lose up to 20% of their bone mass within five to seven years after menopause, making them particularly vulnerable to osteoporotic fractures
| [8] | Ferrari, S. L., Abrahamsen, B., Napoli, N., Akesson, K., Chandran, M., Eastell, R.,... Kanis, J. A. (2016). Diagnosis and management of osteoporosis in postmenopausal women. Nature Reviews Endocrinology, 12(9), 485–496.
https://doi.org/10.1038/nrendo.2016.90 |
[8]
. Although men also experience age-related bone loss, the onset is slower and fracture risk occurs later in life
.
Urban–rural differences in osteoporosis prevalence remain inconsistently reported in developing countries. Urbanization is often associated with sedentary behavior, obesity, and dietary transitions, whereas rural populations may experience chronic undernutrition and limited access to healthcare
. Bangladesh, undergoing rapid urbanization while retaining a large rural population, offers a unique setting to explore these disparities. However, population- based comparative data remain scarce. This study addresses this gap by systematically evaluating bone health across gender, age groups, and residential settings in Bangladesh.
2. Objective
The primary objective of this study was to assess the prevalence of osteopenia and osteoporosis among adults residing in urban and rural regions of Bangladesh using standardized WHO diagnostic criteria
. By quantifying bone health status, the study sought to identify the magnitude of subclinical bone disease within the general adult population.
The secondary objectives were to examine gender- and age-specific differences in bone mineral density and to determine independent predictors of abnormal bone health using multivariable statistical modeling. Additionally, the study aimed to evaluate whether residential setting independently influences bone health after adjusting for demographic factors, thereby informing targeted public health interventions.
3. Materials & Methodology
This cross-sectional analytical study was conducted among adults attending two healthcare facilities: one urban center located in Dhaka and one rural center located in Sylhet. A total sample size of 380 participants was selected, with equal representation from each region to ensure balanced comparison. The study population included both male and female adults aged 18 years and above.
Inclusion Criteria
Participants were eligible if they were aged 18 years or older, had resided in the respective region for a minimum of five years, and provided informed consent. Both symptomatic and asymptomatic individuals were included to capture subclinical disease prevalence.
Exclusion Criteria
Individuals with known metabolic bone diseases other than osteoporosis, chronic kidney disease, malignancy, endocrine disorders affecting bone metabolism, prolonged corticosteroid use, or current pregnancy were excluded to minimize confounding effects.
Data Collection Procedure
Data were collected using a structured questionnaire that captured sociodemographic characteristics, medical history, physical activity levels, and lifestyle factors. Bone mineral density was assessed using standardized measurements, and T-scores and Z-scores were calculated. Bone health status was classified according to WHO criteria as normal, osteopenia, or osteoporosis
.
Statistical Data Analysis
Data analysis was performed using SPSS software. Descriptive statistics summarized participant characteristics. Chi-square tests evaluated associations between categorical variables, while independent t-tests compared mean BMD scores. Pearson correlation analysis assessed relationships between age and BMD scores. Multivariable logistic regression was used to identify independent predictors of abnormal bone health. Model fit was assessed using Hosmer–Lemeshow statistics. A p-value of <0.05 was considered statistically significant.
4. Results
Overall Demographic and Clinical Characteristics
A total of 380 participants were included in the analysis, with equal representation from urban (Dhaka) and rural (Sylhet) regions (n = 190 each). Females constituted the majority of the study population (58.9%), while males accounted for 41.1%. The mean age of participants was 45.3 ± 15.2 years. Nearly two-thirds of the participants reported sedentary physical activity, and a substantial proportion had comorbid conditions such as diabetes mellitus (37.1%) and cardiovascular disease (22.9%).
Table 1. Demographic and Clinical Characteristics of Study Participants (N = 380).
Characteristic | Category | n | % |
Gender | Male | 156 | 41.1 |
Female | 224 | 58.9 |
Age Group | <40 years | 127 | 33.4 |
40–60 years | 168 | 44.2 |
>60 years | 85 | 22.4 |
Residence | Urban (Dhaka) | 190 | 50.0 |
Rural (Sylhet) | 190 | 50.0 |
Bone Health Status | Normal | 74 | 19.5 |
Osteopenia | 276 | 72.6 |
Osteoporosis | 30 | 7.9 |
Distribution of Bone Health Status by Region
Overall, abnormal bone health (osteopenia or osteoporosis) was observed in 306 participants (80.5%). The prevalence of normal bone density was identical in both Dhaka and Sylhet (19.5%). Osteopenia was the most prevalent condition in both regions (72.6%), followed by osteoporosis (7.9%). No statistically significant difference was observed between urban and rural populations (χ² = 0.00, p = 1.000).
Table 2. Bone Health Status Distribution by Region.
Bone Status | Total (N=380) | Sylhet (n=190) | Dhaka (n=190) | p-value |
Normal | 74 (19.5%) | 37 (19.5%) | 37 (19.5%) | 1.000 |
Osteopenia | 276 (72.6%) | 138 (72.6%) | 138 (72.6%) |
Osteoporosis | 30 (7.9%) | 15 (7.9%) | 15 (7.9%) |
Total Abnormal | 306 (80.5%) | 153 (80.5%) | 153 (80.5%) |
Gender-Based Distribution of Bone Health
Marked gender differences were observed in bone health status. Females demonstrated a significantly higher prevalence of abnormal bone health (85.7%) compared to males (73.1%). Osteoporosis prevalence among females (9.8%) was nearly double that observed in males (5.1%). The gender effect was statistically significant (χ² = 15.24, p = 0.001), while regional effects remained non-significant.
Table 3. Bone Health Status by Gender and Region.
Gender / Region | Normal | Osteopenia | Osteoporosis | Total | % Abnormal |
Male – Sylhet | 21 (26.9%) | 53 (68.0%) | 4 (5.1%) | 78 | 73.1 |
Male – Dhaka | 21 (26.9%) | 53 (68.0%) | 4 (5.1%) | 78 | 73.1 |
Female – Sylhet | 16 (14.3%) | 85 (75.9%) | 11 (9.8%) | 112 | 85.7 |
Female – Dhaka | 16 (14.3%) | 85 (75.9%) | 11 (9.8%) | 112 | 85.7 |
Bone Mineral Density Scores
The mean T-score for the total population was −1.84 ± 0.91, while the mean Z-score was −1.21 ± 1.14. No difference was observed between regions. However, females had significantly lower T-scores and Z-scores compared to males (t = 6.87, p < 0.001).
Table 4. Mean Bone Mineral Density Scores by Gender and Region.
Group | n | T-Score (Mean ± SD) | Z-Score (Mean ± SD) |
Total | 380 | −1.84 ± 0.91 | −1.21 ± 1.14 |
Male | 156 | −1.52 ± 0.76 | −0.89 ± 0.97 |
Female | 224 | −2.07 ± 0.94 | −1.43 ± 1.19 |
Age-Stratified Analysis
Bone health deteriorated progressively with advancing age. Participants aged >60 years exhibited the highest prevalence of abnormal bone health (>90%). The age effect was statistically significant (χ² = 24.67, p < 0.001), while region-by-age interaction was not significant.
Table 5. Age-Stratified Bone Health Status by Region.
Age Group | Region | Normal | Osteopenia | Osteoporosis | % Abnormal |
<40 years | Sylhet | 19 (29.7%) | 42 (65.6%) | 3 (4.7%) | 70.3 |
40–60 years | Sylhet | 14 (16.7%) | 61 (72.6%) | 9 (10.7%) | 83.3 |
>60 years | Sylhet | 4 (9.5%) | 35 (83.3%) | 3 (7.2%) | 90.5 |
Correlation and Regression Analysis
Age demonstrated a significant negative correlation with both T-score (r = −0.52) and Z-score (r = −0.48), while T-score and Z-score were strongly positively correlated (r = 0.87; p < 0.001).
Table 6. Pearson Correlation Analysis.
Variables | r | p-value |
Age vs T-Score | −0.52 | <0.001 |
Age vs Z-Score | −0.48 | <0.001 |
T-Score vs Z-Score | 0.87 | <0.001 |
Multivariable logistic regression identified female gender and increasing age as independent predictors of abnormal bone health, while region was not significant.
Table 7. Multivariable Logistic Regression Analysis.
Predictor | Odds Ratio | 95% CI | p-value |
Female gender | 2.27 | 1.42–3.63 | 0.001 |
Age (per year) | 1.06 | 1.04–1.07 | <0.001 |
Region (Dhaka) | 1.00 | 0.62–1.61 | 1.000 |
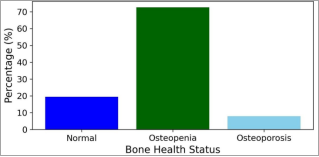
Figure 1. Distribution of Bone Health Status Among Study Participants.
Bar chart illustrating the percentage distribution of bone health status among the study population (N = 380). Bone health was classified according to World Health Organization T- score criteria as normal (T ≥ −1.0), osteopenia (T = −1.0 to −2.5), and osteoporosis (T < −2.5). Osteopenia constituted the largest proportion of cases, followed by normal bone density and osteoporosis.
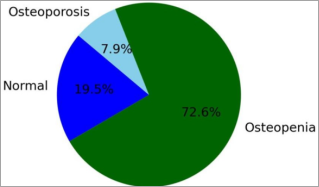
Figure 2. Overall Prevalence of Osteopenia and Osteoporosis.
Pie chart depicting the overall prevalence of normal bone density, osteopenia, and osteoporosis in the study population (N = 380). The figure highlights the predominance of osteopenia, indicating a substantial proportion of individuals at increased risk for progression to osteoporosis.
Summary of Key Findings
In summary, osteopenia and osteoporosis were highly prevalent in this population, with gender and age exerting significant effects on bone health. Regional differences were negligible, indicating that biological and demographic factors outweigh geographic influences.
5. Discussion
The present study reveals an alarmingly high prevalence of osteopenia and osteoporosis among Bangladeshi adults, with more than four-fifths of participants exhibiting abnormal bone mineral density. These findings underscore the silent yet pervasive nature of bone loss in this population and align with reports from other South Asian countries
| [11] | Mithal, A., Bansal, B., Kyer, C. S., & Ebeling, P. (2013). The Asia-Pacific regional audit epidemiology, costs, and burden of osteoporosis. Osteoporosis International, 24(2), 451–458.
https://doi.org/10.1007/s00198-012-1973-0 |
| [12] | Gupta, A. (2015). Osteoporosis in India the nutritional hypothesis. National Medical Journal of India, 28(4), 175–182. |
| [13] | Pasco, J. A., Seeman, E., Henry, M. J., Merriman, E. N., Nicholson, G. C., & Kotowicz, M. A. (2006). The population burden of fractures originates in women with osteopenia. Osteoporosis International, 17(9), 1404–1409.
https://doi.org/10.1007/s00198-006-0135-9 |
[11-13]
.
The predominance of osteopenia over osteoporosis suggests that a large proportion of individuals are at increased risk of progression to osteoporosis if preventive measures are not implemented. Early identification at the osteopenic stage offers a critical opportunity for intervention through lifestyle modification and nutritional supplementation
.
Gender disparity was a prominent finding, with females demonstrating significantly lower bone mineral density and higher osteoporosis prevalence. This observation is consistent with global evidence highlighting the role of estrogen deficiency, lower peak bone mass, and nutritional inadequacies in women
| [7] | Black, D. M., & Rosen, C. J. (2016). Postmenopausal osteoporosis. The New England Journal of Medicine, 374(3), 254–262. https://doi.org/10.1056/NEJMcp1513724 |
| [15] | Leslie, W. D., & Lix, L. M. (2014). Comparison between various fracture risk assessment tools. Current Osteoporosis Reports, 12(3), 353–360.
https://doi.org/10.1007/s11914-014-0224-2 |
[7, 15]
. The particularly high prevalence among postmenopausal women emphasizes the need for gender-sensitive screening programs.
Age-related bone loss emerged as a strong determinant of abnormal bone health. The inverse relationship between age and both T-score and Z-score reflects cumulative skeletal degeneration and reduced bone remodeling capacity with advancing age
| [16] | Looker, A. C., Melton, L. J., Harris, T. B., Borrud, L. G., & Shepherd, J. A. (2010). Prevalence and trends in low femur bone density. Osteoporosis International, 21(1), 1–12.
https://doi.org/10.1007/s00198-009-0942-0 |
[16]
. These findings are consistent with longitudinal studies demonstrating exponential fracture risk increases after the sixth decade of life
.
Interestingly, no significant difference was observed between urban and rural populations. This finding suggests that shared risk factors such as poor nutrition, limited osteoporosis awareness, and lack of routine screening may overshadow geographic influences in Bangladesh. Similar observations have been reported in other developing countries undergoing rapid urbanization
.
6. Limitations of the Study
Despite its strengths, this study has several limitations. The cross-sectional design limits causal inference between risk factors and bone health outcomes. Important variables such as dietary calcium intake, vitamin D status, sunlight exposure, hormonal levels, and fracture history were not assessed. Additionally, the facility-based sampling may limit generalizability to the broader population. Future longitudinal and population-based studies incorporating biochemical markers are recommended.
7. Conclusion
This study provides robust epidemiological evidence demonstrating that osteopenia and osteoporosis constitute a significant and largely underrecognized public health problem among adults in Bangladesh. The exceptionally high prevalence of abnormal bone mineral density, affecting more than four-fifths of the study population, underscores the silent yet pervasive nature of skeletal deterioration in this setting. The predominance of osteopenia over established osteoporosis is particularly noteworthy, as it represents a critical, potentially reversible stage of bone loss that often remains undetected in routine clinical practice
| [1] | Kanis, J. A. (2002). Diagnosis of osteoporosis and assessment of fracture risk. The Lancet, 359(9321), 1929–1936.
https://doi.org/10.1016/S0140-6736(02)08761-5 |
| [2] | World Health Organization. (1994). Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Report of a WHO Study Group. World Health Organization. |
[1, 2]
.
Gender emerged as one of the strongest determinants of bone health in this study. Females exhibited significantly lower mean T-scores and Z-scores and a markedly higher prevalence of both osteopenia and osteoporosis compared to males. These findings are consistent with global literature highlighting the profound impact of estrogen deficiency, reduced peak bone mass, and accelerated postmenopausal bone loss in women
| [7] | Black, D. M., & Rosen, C. J. (2016). Postmenopausal osteoporosis. The New England Journal of Medicine, 374(3), 254–262. https://doi.org/10.1056/NEJMcp1513724 |
| [15] | Leslie, W. D., & Lix, L. M. (2014). Comparison between various fracture risk assessment tools. Current Osteoporosis Reports, 12(3), 353–360.
https://doi.org/10.1007/s11914-014-0224-2 |
[7, 15]
. The disproportionately high prevalence of osteoporosis among older women, particularly those above 60 years of age, highlights an urgent need for gender-sensitive screening strategies and preventive interventions tailored to postmenopausal populations in Bangladesh.
Age-related decline in bone mineral density was another key finding, with a clear and statistically significant inverse relationship observed between age and both T-score and Z-score values. The progressive increase in abnormal bone health across successive age groups reflects cumulative skeletal degeneration and diminished bone remodeling capacity with advancing age
| [16] | Looker, A. C., Melton, L. J., Harris, T. B., Borrud, L. G., & Shepherd, J. A. (2010). Prevalence and trends in low femur bone density. Osteoporosis International, 21(1), 1–12.
https://doi.org/10.1007/s00198-009-0942-0 |
| [17] | Melton, L. J. (2003). Adverse outcomes of osteoporotic fractures in the general population. The Lancet, 361(9371), 192–193. https://doi.org/10.1016/S0140-6736(03)12223-0 |
[16, 17]
. These findings reinforce the importance of early-life and midlife interventions aimed at maximizing peak bone mass and slowing age-related bone loss, thereby reducing fracture risk in later years.
Interestingly, residential setting did not independently influence bone health outcomes. The absence of significant urban–rural differences suggests that shared risk factors such as inadequate nutritional intake, limited awareness of osteoporosis, low physical activity levels, and insufficient access to routine screening may transcend geographic boundaries in Bangladesh. This finding has important public health implications, indicating that osteoporosis prevention strategies should be implemented at a national level rather than being geographically targeted.
From a policy and healthcare perspective, the findings of this study call for the integration of osteoporosis screening into primary healthcare services, particularly for women above 50 years of age and all adults above 60 years. Early identification of osteopenia offers a valuable opportunity
for low-cost interventions, including lifestyle modification, dietary optimization, calcium and vitamin D supplementation, and appropriate pharmacological therapy for high- risk individuals. Such measures have the potential to significantly reduce fracture incidence, healthcare expenditure, and disability associated with osteoporotic fractures.
In conclusion, this study highlights osteoporosis and osteopenia as emerging non- communicable disease priorities in Bangladesh. Addressing this growing burden will require a coordinated, multisectoral approach involving healthcare providers, policymakers, and public health authorities. By shifting the focus from fracture management to early detection and prevention, Bangladesh can mitigate the long-term health and economic consequences of skeletal disorders and improve quality of life for its aging population.
Abbreviations
BMD | Bone Mineral Density |
WHO | World Health Organization |
SD | Standard Deviation |
CI | Confidence Interval |
OR | Odds Ratio |
BMI | Body Mass Index |
SPSS | Statistical Package for the Social Sciences |
χ² | Chi-square Test |
T-score | Bone Density Comparison with Young Adult Reference |
Z-score | Bone Density Comparison with Age-Matched Reference |
Acknowledgments
The authors sincerely acknowledge all study participants for their cooperation and valuable time. We also extend our gratitude to the healthcare professionals and technical staff at the participating centers for their assistance in participant recruitment, data collection, and coordination. Their dedication was instrumental in the successful completion of this research.
Author Contributions
Shanta Saha: Methodology, Project administration, Resources, Software
Md. Alahi Khandaker: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology
Anupam Saha: Formal Analysis, Investigation, Project administration, Software, Validation
Ahmad Zahid Al Quadir: Conceptualization, Funding acquisition, Investigation, Software, Supervision, Validation
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Kanis, J. A. (2002). Diagnosis of osteoporosis and assessment of fracture risk. The Lancet, 359(9321), 1929–1936.
https://doi.org/10.1016/S0140-6736(02)08761-5
|
| [2] |
World Health Organization. (1994). Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Report of a WHO Study Group. World Health Organization.
|
| [3] |
Johnell, O., & Kanis, J. A. (2006). An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis International, 17(12), 1726–1733.
https://doi.org/10.1007/s00198-006-0172-4
|
| [4] |
Compston, J., McClung, M., & Leslie, W. D. (2019). Osteoporosis. The Lancet, 393(10169), 364–376.
https://doi.org/10.1016/S0140-6736(18)32112-3
|
| [5] |
Cauley, J. A. (2013). Public health impact of osteoporosis. The Journals of Gerontology: Series A, 68(10), 1243–1251.
https://doi.org/10.1093/gerona/glt093
|
| [6] |
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. (2001). Osteoporosis prevention, diagnosis, and therapy. JAMA, 285(6), 785–795.
https://doi.org/10.1001/jama.285.6.785
|
| [7] |
Black, D. M., & Rosen, C. J. (2016). Postmenopausal osteoporosis. The New England Journal of Medicine, 374(3), 254–262.
https://doi.org/10.1056/NEJMcp1513724
|
| [8] |
Ferrari, S. L., Abrahamsen, B., Napoli, N., Akesson, K., Chandran, M., Eastell, R.,... Kanis, J. A. (2016). Diagnosis and management of osteoporosis in postmenopausal women. Nature Reviews Endocrinology, 12(9), 485–496.
https://doi.org/10.1038/nrendo.2016.90
|
| [9] |
Eastell, R., Szulc, P., & Compston, J. (2016). Osteoporosis in men. European Journal of Endocrinology, 174(2), R53–R65.
https://doi.org/10.1530/EJE-15-0468
|
| [10] |
Sözen, T., Özışık, L., & Başaran, N. Ç. (2017). An overview and management of osteoporosis. European Journal of Rheumatology, 4(1), 46–56.
https://doi.org/10.5152/eurjrheum.2016.048
|
| [11] |
Mithal, A., Bansal, B., Kyer, C. S., & Ebeling, P. (2013). The Asia-Pacific regional audit epidemiology, costs, and burden of osteoporosis. Osteoporosis International, 24(2), 451–458.
https://doi.org/10.1007/s00198-012-1973-0
|
| [12] |
Gupta, A. (2015). Osteoporosis in India the nutritional hypothesis. National Medical Journal of India, 28(4), 175–182.
|
| [13] |
Pasco, J. A., Seeman, E., Henry, M. J., Merriman, E. N., Nicholson, G. C., & Kotowicz, M. A. (2006). The population burden of fractures originates in women with osteopenia. Osteoporosis International, 17(9), 1404–1409.
https://doi.org/10.1007/s00198-006-0135-9
|
| [14] |
Reginster, J. Y., & Burlet, N. (2006). Osteoporosis: A still increasing prevalence. Bone, 38(2 Suppl 1), S4–S9.
https://doi.org/10.1016/j.bone.2005.11.024
|
| [15] |
Leslie, W. D., & Lix, L. M. (2014). Comparison between various fracture risk assessment tools. Current Osteoporosis Reports, 12(3), 353–360.
https://doi.org/10.1007/s11914-014-0224-2
|
| [16] |
Looker, A. C., Melton, L. J., Harris, T. B., Borrud, L. G., & Shepherd, J. A. (2010). Prevalence and trends in low femur bone density. Osteoporosis International, 21(1), 1–12.
https://doi.org/10.1007/s00198-009-0942-0
|
| [17] |
Melton, L. J. (2003). Adverse outcomes of osteoporotic fractures in the general population. The Lancet, 361(9371), 192–193.
https://doi.org/10.1016/S0140-6736(03)12223-0
|
| [18] |
Harvey, N. C., Dennison, E., & Cooper, C. (2018). Osteoporosis: Impact on health and economics. Nature Reviews Rheumatology, 14(2), 99–109.
https://doi.org/10.1038/nrrheum.2017.208
|
Cite This Article
-
APA Style
Saha, S., Khandaker, M. A., Saha, A., Quadir, A. Z. A. (2026). Gender and Age-specific Patterns of Osteopenia and Osteoporosis in Urban and Rural Bangladesh. International Journal of Medical Research and Innovation, 2(2), 30-36. https://doi.org/10.11648/j.ijmri.20260202.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Saha, S.; Khandaker, M. A.; Saha, A.; Quadir, A. Z. A. Gender and Age-specific Patterns of Osteopenia and Osteoporosis in Urban and Rural Bangladesh. Int. J. Med. Res. Innovation 2026, 2(2), 30-36. doi: 10.11648/j.ijmri.20260202.11
Copy
|
Download
AMA Style
Saha S, Khandaker MA, Saha A, Quadir AZA. Gender and Age-specific Patterns of Osteopenia and Osteoporosis in Urban and Rural Bangladesh. Int J Med Res Innovation. 2026;2(2):30-36. doi: 10.11648/j.ijmri.20260202.11
Copy
|
Download
-
@article{10.11648/j.ijmri.20260202.11,
author = {Shanta Saha and Md. Alahi Khandaker and Anupam Saha and Ahmad Zahid Al Quadir},
title = {Gender and Age-specific Patterns of Osteopenia and Osteoporosis in Urban and Rural Bangladesh},
journal = {International Journal of Medical Research and Innovation},
volume = {2},
number = {2},
pages = {30-36},
doi = {10.11648/j.ijmri.20260202.11},
url = {https://doi.org/10.11648/j.ijmri.20260202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmri.20260202.11},
abstract = {Background: Osteoporosis and osteopenia represent major yet underrecognized public health challenges in low- and middle-income countries. In South Asia, demographic aging, nutritional inadequacies, sedentary lifestyles, and limited access to diagnostic facilities have contributed to a rising burden of bone mineral disorders. Bangladesh, in particular, lacks large comparative studies evaluating bone health across gender and residential settings. Aim: The present study aimed to determine the prevalence of osteopenia and osteoporosis among adults in Bangladesh and to examine the influence of gender, age, and residential setting (urban versus rural) on bone mineral density. Methods: A cross-sectional analytical study was conducted among 380 adults equally sampled from urban Dhaka and rural Sylhet. Bone mineral density was evaluated using WHO-defined T-score and Z-score criteria. Statistical analyses included descriptive statistics, chi-square tests, independent t-tests, Pearson correlation analysis, and multivariable logistic regression to identify independent predictors of abnormal bone health. Results: Abnormal bone mineral density was detected in 80.5% of participants, with osteopenia constituting the majority (72.6%). Females exhibited significantly lower mean T-scores and higher prevalence of osteoporosis compared to males. Age showed a strong inverse correlation with both T-score and Z-score. Gender and age emerged as independent predictors, while residential region showed no significant association. Conclusion: The study highlights a substantial burden of subclinical and clinical bone disease in Bangladesh, particularly among women and older adults. These findings emphasize the need for early screening, preventive interventions, and national osteoporosis control strategies.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Gender and Age-specific Patterns of Osteopenia and Osteoporosis in Urban and Rural Bangladesh
AU - Shanta Saha
AU - Md. Alahi Khandaker
AU - Anupam Saha
AU - Ahmad Zahid Al Quadir
Y1 - 2026/03/05
PY - 2026
N1 - https://doi.org/10.11648/j.ijmri.20260202.11
DO - 10.11648/j.ijmri.20260202.11
T2 - International Journal of Medical Research and Innovation
JF - International Journal of Medical Research and Innovation
JO - International Journal of Medical Research and Innovation
SP - 30
EP - 36
PB - Science Publishing Group
SN - 3070-6319
UR - https://doi.org/10.11648/j.ijmri.20260202.11
AB - Background: Osteoporosis and osteopenia represent major yet underrecognized public health challenges in low- and middle-income countries. In South Asia, demographic aging, nutritional inadequacies, sedentary lifestyles, and limited access to diagnostic facilities have contributed to a rising burden of bone mineral disorders. Bangladesh, in particular, lacks large comparative studies evaluating bone health across gender and residential settings. Aim: The present study aimed to determine the prevalence of osteopenia and osteoporosis among adults in Bangladesh and to examine the influence of gender, age, and residential setting (urban versus rural) on bone mineral density. Methods: A cross-sectional analytical study was conducted among 380 adults equally sampled from urban Dhaka and rural Sylhet. Bone mineral density was evaluated using WHO-defined T-score and Z-score criteria. Statistical analyses included descriptive statistics, chi-square tests, independent t-tests, Pearson correlation analysis, and multivariable logistic regression to identify independent predictors of abnormal bone health. Results: Abnormal bone mineral density was detected in 80.5% of participants, with osteopenia constituting the majority (72.6%). Females exhibited significantly lower mean T-scores and higher prevalence of osteoporosis compared to males. Age showed a strong inverse correlation with both T-score and Z-score. Gender and age emerged as independent predictors, while residential region showed no significant association. Conclusion: The study highlights a substantial burden of subclinical and clinical bone disease in Bangladesh, particularly among women and older adults. These findings emphasize the need for early screening, preventive interventions, and national osteoporosis control strategies.
VL - 2
IS - 2
ER -
Copy
|
Download