The modern method of diagnosis of lung lesions, biopsy guided by CT is widely used in clinical practice. Especially this method is used frequently in oncological hospitals. In our study we analyzed data of patients of the oncology institute, who underwent a lung biopsy using a biopsy guided by CTand complications associated with this diagnostic procedure. The aim of our study was to objectively evaluate the types of complications in patients after the procedure, to compare them with data from the preliminary examination in order to reduce or avoid them in the future. Among all patients who underwent this procedure (89), the number of serious complications during this period of 1.5 years was: pneumothorax 5.6%, hemorrhage 1.1%, hemoptisis - upto 3.3%. In our opinion, the elevation of the risks is influenced by long smoking history (clinical data, coagulation disorders). We discuss in detail the tactics of management and observation of patients after the procedure, taking into account the patient's medical history and complications during the procedure. Careful preliminary preparation of the patients before the procedure helps to reduce the risk of complications.
| Published in | International Journal of Pharmacy and Chemistry (Volume 12, Issue 2) |
| DOI | 10.11648/j.ijpc.20261202.11 |
| Page(s) | 19-23 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
CT, Lung Biopsy Guided by CT, Lung Injury, Pneumothorax, Pulmonary Hemorrhage/Hemoptysis
Lymphoma | Atypical | Noduls with ≤5mm | 5-10mm | 11-20mm | ≥20mm | Quantity | |
|---|---|---|---|---|---|---|---|
Benign | 9 | 4 | 8 | 9 | 30 | ||
Malignant | 3 | 2 | 1 | 12 | 32 | 50 | |
Metastases | 3 | 3 | 3 | 9 | |||
Quantity | 3 | 11 | 7 | 23 | 44 | 89 |
Complications | Number |
|---|---|
Pneumothorax (serious) | 5 cases |
Alveolar hemorrhage (severe) | 1 case |
Hemoptysis (serious) | 3 cases |
Death | 1 case |
BUN | Blood Urea Nitrogen |
CBC | Complete Blood Count |
CT | Computer Tomography |
HIV | Human Immunodeficiency Virus |
MRI | Magnetic Resonance Imaging |
PET | Positron Emission Tomography |
| [1] | Mir MF, Naik MA, Mali JA. CT guided lung biopsy complications: a single center prospective study. Int J Res Med Sci. 2018 Sep; 6(9): 2946. |
| [2] | Heerink WJ, de Bock GH, de Jonge GJ, et al. Complication rates of CT-guided transthoracic lung biopsy: meta-analysis. Eur Radiol. 2017; 27: 138-148. |
| [3] | Otto S., Mensel B., Friedrich N., et al. Predictors of technical success and rate of complications of image-guided percutaneous transthoracic lung needle biopsy of pulmonary tumors. PLoS One. 2015 Apr 9; 10(4): e0124947. |
| [4] | Dezube R. Transthoracic Needle Biopsy. Johns Hopkins University; Nov 2023. |
| [5] | Villegas J., Moreno L., Piedrahita M. Complications of percutaneous biopsy of lung guided by ct scan. Rev According To Columbus Radiol. 2021; 32(3): 5584-90. |
| [6] | Kharchenko VP, Glagolev NA. Computed tomography X-ray in the diagnosis of diseases of the lungs and the mediastinum. Medika; 2005: 120. |
| [7] | Chernousov AF, Pavlov YV, Pavlov AYu. Diagnosis and treatment of small formations pulmonary peripheral. Surgery. 2010; 6: 61-69. |
| [8] | Ragulin YA, Usachev VS, Medvedev VN, et al. The CT-guided transthoracic biopsy of lung and mediastinal tumors. Medical Radiological Research Center of the Ministry of Health and Social Development of Russia, Obninsk. |
| [9] | Manhire A, Charig M, Clelland C, Gleeson F, Miller R, Moss H, Pointon K, Richardson C, Sawicka E; Guidelines for radiologically guided lung biopsy. Thorax. 2003 Nov; 58 (11): 920-36. |
| [10] | Herf S. M, Suratt P. M, Arora N. S Deaths and complications associated with transbronchial lung biopsy. Am Rev Respir Dis. 1977 Apr; 115(4): 708-11. |
| [11] | Han Y, Kim HJ, Kong KA, Kim SJ, Lee SH, Ryu YJ, Lee JH. Kim Y, Shim SS, Chang JH. Diagnosis of small pulmonary lesions by transbronchial lung biopsy with radial endobronchial ultrasound and virtual bronchoscopic navigation versus CT-guided transthoracic needle biopsy: A systematic review and meta-analysis. PLoS One. 2018 Jan 22; 13(1). |
| [12] | Hu Y, Yang X, Nie L, Zhao D, An J, Li B. Analysis of Clinical Characteristics and Driver Genes in 405 Patients with Lung Cancer Complicated with Tuberculosis. Zhongguo Fei Ai Za Zhi 2020 May 20; 23(5): 337-342. |
| [13] | Jurczak P, Romaszko-Wojtowicz A, Doboszyńska A. Lung Lesions: Differential Diagnoses Beyond Cancer. Am J Case Rep. 2024 Jun 15: 25: e943798. |
| [14] | Ramón Rami-Porta, Hisao Asamura, William D Travis, Valerie W Rusch. Lung cancer - major changes in the American Joint Committee on Cancer eighth edition cancer staging manual CA Cancer J Clin. 2017 Mar; 67(2): 138-155. |
| [15] | Arash Najafi, Marc Al Ahmar, Baptiste Bonnet, Alexandre Delpla, Adrian Kobe, Khaled Madani, Charles Roux, Frédéric Deschamps, Thierry de Baère, Lambros Tselikas. The PEARL Approach for CT-guided Lung Biopsy: Assessment of Complication Rate. Radiology. 2022 Feb; 302(2): 473-480. |
APA Style
Krylova, A., Rudinskiy, K., Alba, V. (2026). A Review of CT-Guided Lung Biopsy: Procedure Stages, Complications, and Risk Mitigation. International Journal of Pharmacy and Chemistry, 12(2), 19-23. https://doi.org/10.11648/j.ijpc.20261202.11
ACS Style
Krylova, A.; Rudinskiy, K.; Alba, V. A Review of CT-Guided Lung Biopsy: Procedure Stages, Complications, and Risk Mitigation. Int. J. Pharm. Chem. 2026, 12(2), 19-23. doi: 10.11648/j.ijpc.20261202.11
@article{10.11648/j.ijpc.20261202.11,
author = {Anna Krylova and Kirill Rudinskiy and Venecia Alba},
title = {A Review of CT-Guided Lung Biopsy: Procedure Stages, Complications, and Risk Mitigation},
journal = {International Journal of Pharmacy and Chemistry},
volume = {12},
number = {2},
pages = {19-23},
doi = {10.11648/j.ijpc.20261202.11},
url = {https://doi.org/10.11648/j.ijpc.20261202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijpc.20261202.11},
abstract = {The modern method of diagnosis of lung lesions, biopsy guided by CT is widely used in clinical practice. Especially this method is used frequently in oncological hospitals. In our study we analyzed data of patients of the oncology institute, who underwent a lung biopsy using a biopsy guided by CTand complications associated with this diagnostic procedure. The aim of our study was to objectively evaluate the types of complications in patients after the procedure, to compare them with data from the preliminary examination in order to reduce or avoid them in the future. Among all patients who underwent this procedure (89), the number of serious complications during this period of 1.5 years was: pneumothorax 5.6%, hemorrhage 1.1%, hemoptisis - upto 3.3%. In our opinion, the elevation of the risks is influenced by long smoking history (clinical data, coagulation disorders). We discuss in detail the tactics of management and observation of patients after the procedure, taking into account the patient's medical history and complications during the procedure. Careful preliminary preparation of the patients before the procedure helps to reduce the risk of complications.},
year = {2026}
}
TY - JOUR T1 - A Review of CT-Guided Lung Biopsy: Procedure Stages, Complications, and Risk Mitigation AU - Anna Krylova AU - Kirill Rudinskiy AU - Venecia Alba Y1 - 2026/07/03 PY - 2026 N1 - https://doi.org/10.11648/j.ijpc.20261202.11 DO - 10.11648/j.ijpc.20261202.11 T2 - International Journal of Pharmacy and Chemistry JF - International Journal of Pharmacy and Chemistry JO - International Journal of Pharmacy and Chemistry SP - 19 EP - 23 PB - Science Publishing Group SN - 2575-5749 UR - https://doi.org/10.11648/j.ijpc.20261202.11 AB - The modern method of diagnosis of lung lesions, biopsy guided by CT is widely used in clinical practice. Especially this method is used frequently in oncological hospitals. In our study we analyzed data of patients of the oncology institute, who underwent a lung biopsy using a biopsy guided by CTand complications associated with this diagnostic procedure. The aim of our study was to objectively evaluate the types of complications in patients after the procedure, to compare them with data from the preliminary examination in order to reduce or avoid them in the future. Among all patients who underwent this procedure (89), the number of serious complications during this period of 1.5 years was: pneumothorax 5.6%, hemorrhage 1.1%, hemoptisis - upto 3.3%. In our opinion, the elevation of the risks is influenced by long smoking history (clinical data, coagulation disorders). We discuss in detail the tactics of management and observation of patients after the procedure, taking into account the patient's medical history and complications during the procedure. Careful preliminary preparation of the patients before the procedure helps to reduce the risk of complications. VL - 12 IS - 2 ER -
Innova Clinic Punta Cana, Punta Cana, Dominican Republic
Innova Clinic Punta Cana, Punta Cana, Dominican Republic
Calle C Ensanche, Edificio Isabelita, Santo Domingo Este, Dominican Republic
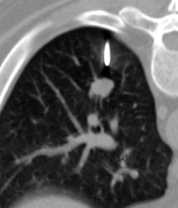
Figure 1. The distance between the lesion and needle.
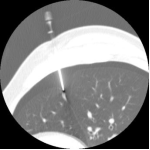
Figure 2. CT-guided transthoracic needle biopsy of a pulmonary lesion.
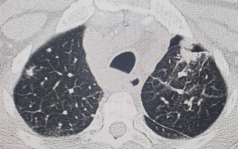
Figure 3. Patient with pneumothorax after the biopsy.
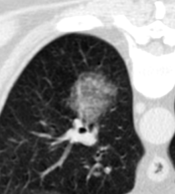
Figure 4. Patient with bleeding after the biopsy.

Figure 5. Lesion before the biopsy.

Figure 6. Injury after the biopsy with findings of hemorrhage.
Information

