Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) continue to devastate the world, particularly women in middle and low-income countries, especially in sub-Saharan Africa. This is principally because it is twofold, that is, gender and context, and thus the infection patterns differ across the gender divide because of biology, physiology, socially constructed gender norms, roles, unequal power relations and social-economic inequalities. The objective of the study was to investigate the efficacy of intervention strategies mitigating the challenges faced by women living with HIV and AIDS in Majengo informal urban settlements in Nyeri County. The study used the descriptive survey design that utilised qualitative and quantitative approaches. Data from participants was collected using the snowballing method and involved in-depth interviews, structured questionnaires and focus group discussions. The study adopted the social systems theory to incorporate consciousness and phenomenology in the construction of society, such as social-economic factors that significantly influence sexual behaviour. The study assessed knowledge and use of preventive measures against sexually transmitted infections (STIs) among infected women and identified risky practices and appropriate strategies for curbing the spread of the virus. The inquiry established that the success of the HIV and AIDS intervention strategies depends largely on context-specific challenges facing various populations, such as women living with HIV and AIDS in informal urban settlements. It recommends adoption of HIV and AIDS intervention strategies that mitigate gender and context-specific challenges in informal settlements, including improved infrastructure and enhanced health.
| Published in | Science Journal of Public Health (Volume 14, Issue 1) |
| DOI | 10.11648/j.sjph.20261401.11 |
| Page(s) | 1-13 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Gender, Women, HIV and AIDS, Informal Urban Settlements, Interventions
Number | Percentage | ||
|---|---|---|---|
Age | 15 - 25 years | 2 | 3.4% |
26 - 35 years | 16 | 27.6% | |
36 - 45 years | 27 | 46.6% | |
46 - 55 years | 9 | 15.5% | |
56 years and over | 4 | 6.9% | |
Total | 58 | 100.0% | |
Occupation | Employed | 20 | 34.5% |
Not employed | 13 | 22.4% | |
Business (self-employed) | 25 | 43.1% | |
Total | 58 | 100.0% | |
Number of Children | 1 - 3 children | 43 | 74.1% |
4 – 7 children | 12 | 20.7% | |
8 - 10 children | 3 | 5.2% | |
Total | 58 | 100.0% | |
Marital Status | Single | 19 | 32.8% |
Married | 22 | 37.9% | |
Divorced | 6 | 10.3% | |
Separated | 11 | 19.0% | |
Total | 58 | 100.0% | |
Unmarried Participants with Partners | Yes | 26 | 68.4% |
No | 12 | 31.6% | |
Total | 38 | 100.0% | |
Level of Education | Primary Level | 35 | 60.3% |
Secondary Level | 13 | 22.4% | |
Tertiary Level | 10 | 17.3% | |
Total | 58 | 100.0% | |
Monthly Income | 1,000 – 3,000 | 15 | 25.9% |
3,000 – 5,000 | 14 | 24.1% | |
5,000 and above | 29 | 50.0% | |
Total | 45 | 100.0% |
Number | Percentage | ||
|---|---|---|---|
Participants given Prophylaxis Drugs at Antenatal Clinic | Yes | 36 | 100.0% |
No | 0 | 0.0% | |
Total | 36 | 100.0% | |
Delivery of First Child in a Health Facility | Yes | 50 | 86.2% |
No | 8 | 13.8% | |
Total | 58 | 100.0% | |
Knowledge by Spouse of Participants’ Status for Married participants | Yes | 16 | 72.7% |
No | 6 | 27.3% | |
Total | 22 | 100.0% | |
Use of Protection (condoms) Every Time Participants Have Sex (Married) | Yes | 3 | 13.6% |
No | 19 | 86.4% | |
Total | 22 | 100.0% | |
Use of Protection Every Time Participants have sex (Partners) | Yes | 9 | 36.0% |
No | 16 | 64.0% | |
Total | 25 | 100.0% |
AIDS | Acquired Immunodeficiency Syndrome |
ART | Anti-retroviral Therapy |
HAPCA | HIV and AIDS Prevention and Control Act |
HEI | HIV Exposed Infants |
HIV | Human Immunodeficiency Virus |
NASCOP | National AIDS and STI Control Programme |
PLHIV | Persons Living with HIV |
PMTCT | Prevention of Mother-to-Child Transmission |
PrEP | Pre-exposure Prophylaxis |
| [1] | Ambert, C., & Msimang, S. (2004). The Tyranny of the Result: A Retrospective and a way forward on Gender, HIV and Aids in Development. Consultants Report to the UNISRID. |
| [2] | American Psychological Association (2024). APA Research Ethics Code: A Guide to Ethical Standards in Research. American Psychological Association. |
| [3] |
Avert, the Global information and education on HIV and AIDS (2021a). HIV and AIDS in Kenya.
https://www.avert.org/global-hiv-and-aids-statistics , downloaded on 24th January 2021. |
| [4] |
Avert, the Global information and education on HIV and AIDS (2021b). HIV and AIDS in Kenya.
https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/kenya downloaded on 24th January 2021. |
| [5] | Berger, J. (2004). Re-sexualising the epidemic: desire, risk and HIV prevention. Development Update: 5(3): 45-67. Interfund, Braamfontein. |
| [6] | British Psychological Society (2021). BPS Code of Human Research Ethics. Leicester: The British Psychological Society. |
| [7] | Bryman, A. & Bell, E. (2015). Business Research Method. Oxford: Oxford University Press. |
| [8] | Bwisa, D. M. (2009). Barriers to the uptake of Prevention of Mother-To Child Transmission (PMTCT) of HIV interventions among women in Kibera slum, Kenya. Unpublished Master thesis, Nairobi: Kenyatta University. |
| [9] | Cicourel, A. V. (2017). The acquisition of social structure: Toward a developmental sociology of language and meaning. Routledge. |
| [10] | Clay, P. G. (2005). The complete HIV/AIDS resource. Supplement Introduction. Available at |
| [11] | Creswell, J. W. & Creswell, J. D. (2017). Research design: Qualitative, quantitative, and mixed methods approaches. Sage publications. |
| [12] | Dawson, C. (2009). Introduction to Research Methods. Oxford University Press. |
| [13] | Dawson, C. (2019). Introduction to Research Methods A Practical Guide for Anyone Undertaking a Research Project. Robinson. |
| [14] | Edwards, K. M., Changilwa, P., Waterman, E., Bikeri, C., Mweru, C., Khayanje, N., & Obel, P. (2021). A promising approach to preventing gender-based violence and HIV among slum-dwelling youth in Nairobi, Kenya, Violence against women, 10778012211014562. |
| [15] | Gliem, J. A., & Gliem, R. R. (2003). Calculating, interpreting, and reporting Cronbach’s alpha reliability coefficient for Likert-type scales. Midwest Research-to-Practice Conference in Adult, Continuing, and Community Education, 82 - 88. |
| [16] | Goodman, L. (1961). Snowball sampling. Annals of Mathematical Statistics 32, 245–268. |
| [17] | Gupta, J. (2000). Gender Sexuality and HIV/AIDS; Plenary address prepared for the XIIIth International AIDS conference organised by the International Centre for Research on Women Durban South Africa. |
| [18] | Hawkins, K., Mussà, F. & Abuxahama, S. (2005). Milking the Cow’ – Young women’s constructions of identity, gender, power and risk in transactional and cross-generational sexual relationships: Maputo, Mozambique. The Implications for Behaviour Change Interventions, Options. Consultancy Services and Populations Services International (PSI), Mozambique. |
| [19] | Ireri, S., Esekon, J. & Kinyua, M. (2024). A Generalized Linear Model of HIV/AIDS Patients in Kenya: A Case Study of Nyeri County Referral Hospital. American Journal of Theoretical and Applied Statistics, 13(4), 80 - 84. |
| [20] | Kenya AIDS Indicator Survey (2007). Data on HIV prevalence according to regions in Kenya. Nairobi: National AIDS Control Council. |
| [21] | Kenya AIDS Indicator Survey (2013). A Preliminary Report. Nairobi: National AIDS Control Council. Nairobi: National AIDS Control Council. |
| [22] | Khan, S. (2020). Examining HIV/AIDS-Related Stigma at Play: Power, Structure, and Implications for HIV Interventions. Health Communication, 35(12), 1509 – 1519. |
| [23] | Kibui, M. (1998). Factors contributing to HIV and AIDS infection in Majengo Urban informal settlements of Nyeri Municipality of Nyeri District. Unpublished Dissertation. KMTC. |
| [24] | Latkin, C., Weeks, M. R., Glasman, L., Galletly, C. & Albarracin, D. (2010). A dynamic social systems model for considering structural factors in HIV prevention and detection. AIDS Behaviour, 14 (Suppl 2): 222 – 238. |
| [25] | Lee, D. B. & Brosziewski, A. (2009). Observing Society: Meaning, Communication, and Social Systems. Cambria Press. |
| [26] | Luhmann, N. (1995). Social Systems. Stanford University Press. |
| [27] | Luhmann, N. (2012a). Introduction to Systems Theory. Polity. |
| [28] | Luhmann, N. (2012b). Theory of Society, Vol. 1. Stanford University Press. |
| [29] | Luhmann, N. (2013). Theory of Society, Vol. 2. Stanford University Press. |
| [30] | Mabaso, M., Makola, L., Naidoo, I., Mlangeni, L. L., Jooste, S., & Simbayi, L. (2019). HIV prevalence in South Africa through gender and racial lenses: results from the 2012 population-based national household survey. International Journal for Equity in Health, 18(1), 1 - 11. |
| [31] | Macaulay, L., Kitzinger, J., Green, G. & Wight, D. (1995). Unconventional conceptions and HIV. Aids Care, 7, 261 - 276. |
| [32] | Madise, J. N., Zibara, K. A., Inungu. J., Khamadi, S. A., Ezeh. A., Zulu. M. E., KebasoJ., Okoth. V., Mwau. M. (2008). Are Slum Dwellers at heightened risk of HIV infection than other urban residents? Evidence from a population-based HIV prevalence surveys in Kenya. Health and Place, 18, 1144 - 1152. |
| [33] | Mathai, L. M., Bururia, D., & Kagema, D. N. (2019). Assessment of Religious Initiated Programmes as Intervention Mechanisms in curbing HIV/AIDS pandemic in Kenya: Some Selected programmes in Meru South Sub-County. Educational Review: International Journal, 16(1), 113-124. |
| [34] | National AIDS and STI Control Programme, NASCOP (2014a). National Guidelines for HIV/STI Programming with Key Populations. Nairobi: Ministry of Health. |
| [35] | National AIDS and STI Control Programme, NASCOP (2014b). Guidelines on Use of Antiretroviral Drugs for Treating and Preventing HIV Infection in Kenya, 2018. Nairobi: Ministry of Health. |
| [36] | National AIDS and STI Control Programme, NASCOP (2022). Kenya HIV Prevention and Treatment Guidelines, 2022. Nairobi: Ministry of Health. |
| [37] | Nyeri District Strategic Plan (2005 – 2010). National coordination agency for population and development. Nyeri Country Government and Ministry of Planning and National Development. Nyeri: District Strategic Plan. |
| [38] | Nyindo, M. (2005). Complementary factors contributing to the rapid spread of HIV-1 in sub- Saharan Africa. A review. East African Medical Journal, 82(1) 40 - 46. |
| [39] | Nzioka, C. (2000). The social meanings of death from HIV/AIDS: An African interpretative view. Culture, Health & Sexuality, 2(1), 1 - 14. |
| [40] | Oliva, R. (2019). Intervention as a research strategy. Journal of Operations Management, 65(7): 710 - 724. |
| [41] | Ojowi, A. L. (2008). Barriers to Safe Obstetric Practices in Prevention of Mother to Child Transmission in Kibera urban informal settlements, Nairobi, Kenya. Master Thesis. Kenyatta University. |
| [42] | Ombati, S. (2019). Factors Influencing the Spread of HIV/AIDS within the Maasai Community of Narok in Kenya and Stigma in the Society. Master Thesis, Arcada University of Applied Sciences. |
| [43] | Pandey, A. & Galvani, A. (2019). The global burden of HIV and prospects for control. The Lancet, 6(12), e809-e811. |
| [44] | Patterson, H. (2011). HIV/AIDS in the slums of Kenya: intervening through effectively utilising volunteers. Published thesis. University of Pittsburgh. |
| [45] | Republic of Kenya (2001). Ministry of Health; Access to HIV-related drugs. Nairobi: Ministry of Health. |
| [46] | Republic of Kenya (2007). Kenya National Guidelines on Nutrition and HIV/AIDS. Nairobi: Ministry of Health. |
| [47] | Republic of Kenya (2014). Kenya AIDS Response Progress Report 2014: Progress towards Zero. Nairobi: Ministry of Health. |
| [48] | Republic of Kenya (2015). Kenya AIDS Strategic Framework 2014/2015 - 2018/2019. Nairobi: Ministry of Health. |
| [49] | Republic of Kenya (2016). Kenya Aids Response Progress Report, 2016. Nairobi: Ministry of Health. |
| [50] | Republic of Kenya (2018). Kenya Health Sector Strategic Plan (KHSSP) of 2018/2019 – 2022/2023. Nairobi: Ministry of Health. |
| [51] | Republic of Kenya (2020). The Kenya AIDS Strategic Framework (KASF II) (2020/2021 – 2024/2025). Nairobi: Ministry of Health. |
| [52] | Republic of Kenya (2023). Kenya Demographic and Health Survey 2022: Key Indicators Report. Nairobi: Ministry of Health. |
| [53] | Ritchie, K. (2020). Social structures and the ontology of social groups. Philosophy and Phenomenological Research, 100(2), 402 - 424. |
| [54] | Rutledge, J. D. (2023). Exploring the role of empowerment in Black women's HIV and AIDS activism in the United States: An integrative literature review. American Journal of Community Psychology, 71(3-4): 491 - 506. |
| [55] | Shamu, S., Khupakonke, S., Farirai, T., Slabbert, J., Chidarikire, T., Guloba, G., & Nkhwashu, N. (2020). Knowledge, attitudes and practices of young adults towards HIV prevention: an analysis of baseline data from a community-based HIV prevention intervention study in two high HIV burden districts, South Africa. BMC Public Health, 20(1), 1 - 10. |
| [56] | Sharma, V., Leight, J., Verani, F., Tewolde, S., & Deyessa, N. (2020). Effectiveness of a culturally appropriate intervention to prevent intimate partner violence and HIV transmission among men, women, and couples in rural Ethiopia: findings from a cluster-randomised controlled trial. PLoS Medicine, 17(8), 1 - 28. |
| [57] | Ting, H., Memon, M. A., Thurasamy, R., & Cheah, J.-H. (2025). Snowball Sampling: A Review and Guidelines for Survey Research. Asian Journal of Business Research, 15(1), 1 – 15. |
| [58] | Turner, J. H., & Abrutyn, S. (2017). Returning the “social” to evolutionary sociology: Reconsidering Spencer, Durkheim, and Marx’s models of “natural” selection. Sociological Perspectives, 60(3), 529 - 556. |
| [59] | Törnävä, M., Palonen, M., Harju, E., Haapa, T., Rissanen, M. & Kylmä, J. (2025). Hard- To-Reach and Hidden Groups in Health-Related Research - A Scoping Review. Journal of Advanced Nursing. 81(9), 5793 - 5805. |
| [60] |
UNAIDS (2017).’Ending AIDS: Progress towards 90-90-90 targets, retrieved from
http://www.unaids.org/en/resources/documents/2017/20170720_Global_AIDS_update_2017 |
| [61] |
UNAIDS (2022a). Fact Sheet, 2022.
https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf , downloaded, 1st March 2023. |
| [62] | UNAIDS (2022b). UNAIDS Global AIDS Update 2022. Joint United Nations Programme on HIV/AIDS (UNAIDS). |
| [63] | Walliman, N. (2010). Research Methods: The Basics. London: Routledge. |
| [64] | Wango, G. M. (2001). The Vulnerability of Girls and Women to HIV/AIDS in Kenya. Unpublished Paper. |
| [65] | Wango, G. M. (2015). Psychological Counselling in Kenya: A Contemporary Review of the Developing World. Nairobi: Kenya Literature Bureau. |
| [66] | Wango, G. M., Wairire, G., & Kimamo, C. (2020). Anxiety and Emotions of COVID-19: The Emotional underpinnings of dealing with the Corona Virus Disease. Journal of Psychology and Behavioural Science, 8(2), 1 - 18. |
| [67] | Wanjiru, S. (2022). Efficacy of Strategies that Mitigate Challenges faced by Women infected with HIV / AIDS in Majengo Urban Informal Settlement, Nyeri County, Kenya. Nairobi: Kenyatta University. |
| [68] |
World Health Organization (2021). HIV/AIDS.
https://www.who.int/news-room/fact-sheets/detail/hiv-aids , downloaded, 25th January 2021. |
| [69] |
World Health Organization (2023). HIV-AIDS: The Global Health Observatory.
https://www.who.int/data/gho/data/themes/hiv-aids , downloaded, 1st March 2023. |
| [70] | Zulu, E. M., Dodo, F., & Ezeh. A. (2003). Urbanisation, Poverty and Sex: Roots of risky sexual behaviour in the Slum Settlements in Nairobi, Kenya. Blackwell Publishing. |
APA Style
Wanjiru, S., Wango, G., Okemwa, P. (2026). Towards and Twofold: Efficacy of HIV Intervention Strategies That Mitigate Challenges for Women in an Urban Informal Settlement, Kenya. Science Journal of Public Health, 14(1), 1-13. https://doi.org/10.11648/j.sjph.20261401.11
ACS Style
Wanjiru, S.; Wango, G.; Okemwa, P. Towards and Twofold: Efficacy of HIV Intervention Strategies That Mitigate Challenges for Women in an Urban Informal Settlement, Kenya. Sci. J. Public Health 2026, 14(1), 1-13. doi: 10.11648/j.sjph.20261401.11
AMA Style
Wanjiru S, Wango G, Okemwa P. Towards and Twofold: Efficacy of HIV Intervention Strategies That Mitigate Challenges for Women in an Urban Informal Settlement, Kenya. Sci J Public Health. 2026;14(1):1-13. doi: 10.11648/j.sjph.20261401.11
@article{10.11648/j.sjph.20261401.11,
author = {Sarah Wanjiru and Geoffrey Wango and Pacificah Okemwa},
title = {Towards and Twofold: Efficacy of HIV Intervention Strategies That Mitigate Challenges for Women in an Urban Informal Settlement, Kenya},
journal = {Science Journal of Public Health},
volume = {14},
number = {1},
pages = {1-13},
doi = {10.11648/j.sjph.20261401.11},
url = {https://doi.org/10.11648/j.sjph.20261401.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20261401.11},
abstract = {Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) continue to devastate the world, particularly women in middle and low-income countries, especially in sub-Saharan Africa. This is principally because it is twofold, that is, gender and context, and thus the infection patterns differ across the gender divide because of biology, physiology, socially constructed gender norms, roles, unequal power relations and social-economic inequalities. The objective of the study was to investigate the efficacy of intervention strategies mitigating the challenges faced by women living with HIV and AIDS in Majengo informal urban settlements in Nyeri County. The study used the descriptive survey design that utilised qualitative and quantitative approaches. Data from participants was collected using the snowballing method and involved in-depth interviews, structured questionnaires and focus group discussions. The study adopted the social systems theory to incorporate consciousness and phenomenology in the construction of society, such as social-economic factors that significantly influence sexual behaviour. The study assessed knowledge and use of preventive measures against sexually transmitted infections (STIs) among infected women and identified risky practices and appropriate strategies for curbing the spread of the virus. The inquiry established that the success of the HIV and AIDS intervention strategies depends largely on context-specific challenges facing various populations, such as women living with HIV and AIDS in informal urban settlements. It recommends adoption of HIV and AIDS intervention strategies that mitigate gender and context-specific challenges in informal settlements, including improved infrastructure and enhanced health.},
year = {2026}
}
TY - JOUR T1 - Towards and Twofold: Efficacy of HIV Intervention Strategies That Mitigate Challenges for Women in an Urban Informal Settlement, Kenya AU - Sarah Wanjiru AU - Geoffrey Wango AU - Pacificah Okemwa Y1 - 2026/01/19 PY - 2026 N1 - https://doi.org/10.11648/j.sjph.20261401.11 DO - 10.11648/j.sjph.20261401.11 T2 - Science Journal of Public Health JF - Science Journal of Public Health JO - Science Journal of Public Health SP - 1 EP - 13 PB - Science Publishing Group SN - 2328-7950 UR - https://doi.org/10.11648/j.sjph.20261401.11 AB - Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS) continue to devastate the world, particularly women in middle and low-income countries, especially in sub-Saharan Africa. This is principally because it is twofold, that is, gender and context, and thus the infection patterns differ across the gender divide because of biology, physiology, socially constructed gender norms, roles, unequal power relations and social-economic inequalities. The objective of the study was to investigate the efficacy of intervention strategies mitigating the challenges faced by women living with HIV and AIDS in Majengo informal urban settlements in Nyeri County. The study used the descriptive survey design that utilised qualitative and quantitative approaches. Data from participants was collected using the snowballing method and involved in-depth interviews, structured questionnaires and focus group discussions. The study adopted the social systems theory to incorporate consciousness and phenomenology in the construction of society, such as social-economic factors that significantly influence sexual behaviour. The study assessed knowledge and use of preventive measures against sexually transmitted infections (STIs) among infected women and identified risky practices and appropriate strategies for curbing the spread of the virus. The inquiry established that the success of the HIV and AIDS intervention strategies depends largely on context-specific challenges facing various populations, such as women living with HIV and AIDS in informal urban settlements. It recommends adoption of HIV and AIDS intervention strategies that mitigate gender and context-specific challenges in informal settlements, including improved infrastructure and enhanced health. VL - 14 IS - 1 ER -
Department of Gender and Development Studies, Kenyatta University, Nairobi, Kenya
Department of Psychology, University of Nairobi, Nairobi, Kenya
Department of Gender and Development Studies, Kenyatta University, Nairobi, Kenya
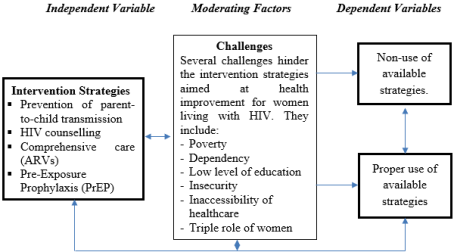
Figure 1. Conceptual Framework on Factors That Lead to Non-Improvement of the Status of Women Infected With HIV.
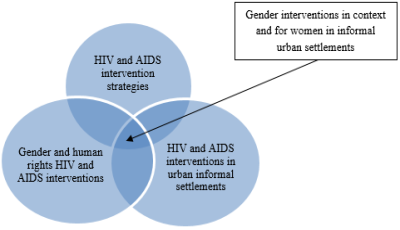
Figure 2. HIV and AIDS Interventions in Sub-Saharan Africa Incorporating Gender.
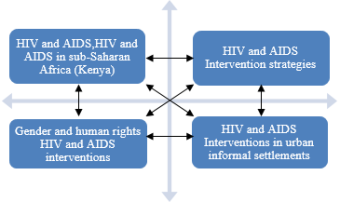
Figure 3. HIV and AIDS and Enhanced Intervention Programmes that Incorporates Gender and Human Rights.
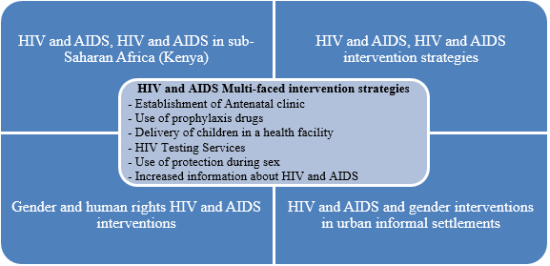
Figure 4. HIV and AIDS Intervention Programmes Characteristics and Context.
Information

