Patients with diabetic foot often have multiple cardio-renal and metabolic comorbidities, which increase perioperative risk, especially in resource-limited settings where ankle block anesthesia is commonly used. The aim of the present study was to identify clusters of these comorbidities in high-risk diabetic patients undergoing foot surgery with ankle block anesthesia and to study correlations among key clinical parameters relevant to perioperative risk. A retrospective correlational study was performed on 71 adult diabetic patients who underwent foot surgery with ankle block anesthesia at Diabetic General Hospital, Chattogram, Bangladesh. Demographic and clinical data, encompassing biochemical, haematologic, renal, and cardiac parameters, were obtained from hospital records. Spearman's rank correlation, principal component analysis (PCA), and hierarchical clustering were used to find patterns of multimorbidity. There were strong links between renal and metabolic variables. Serum creatinine (SC) exhibited a robust inverse correlation with estimated glomerular filtration rate (eGFR), whereas bicarbonate showed a negative correlation with creatinine, indicating a potential link between metabolic acidosis and renal dysfunction. Positive correlations between electrolytes, albumin, and hemoglobin signify homeostatic equilibrium. PCA identified two principal axes-metabolic-electrolyte integrity and renal dysfunction-that encompassed the majority of the variance. Hierarchical clustering delineated three distinct physiological groupings. These results emphasize the necessity for thorough preoperative assessment and multidisciplinary management to enhance perioperative outcomes in this high-risk population. Prospective studies are necessary to enhance risk assessment methodologies.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 14, Issue 2) |
| DOI | 10.11648/j.ijacm.20261402.11 |
| Page(s) | 115-126 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Diabetic Foot, Cardio-renal Syndrome, Chronic Kidney Disease, Ankle Block Anesthesia, Perioperative Risk
Age (Years) | Hb% | Albumin Level | Na+ | K+ | Cl- | HCO3 | Serum Creatinine | GFR | ||
|---|---|---|---|---|---|---|---|---|---|---|
Age (Years) | Spearman Corr. | 1 | 0.07297 | -0.02863 | 0.31516 | 0.20939 | 0.19574 | -0.09797 | 0.16848 | -0.23618 |
p-value | -- | 0.53954 | 0.80996 | 0.00661 | 0.07542 | 0.09939 | 0.40961 | 0.15419 | 0.04426 | |
Hb% | Spearman Corr. | 0.07297 | 1 | 0.12139 | 0.21767 | 0.03685 | 0.31182 | 0.06046 | -0.13672 | 0.18751 |
p-value | 0.53954 | -- | 0.30628 | 0.06432 | 0.75693 | 0.00767 | 0.61137 | 0.24875 | 0.11217 | |
Albumin Level | Spearman Corr. | -0.02863 | 0.12139 | 1 | 0.1703 | 0.33751 | 0.03016 | 0.13798 | -0.17192 | 0.1023 |
p-value | 0.80996 | 0.30628 | -- | 0.14973 | 0.0035 | 0.80144 | 0.24438 | 0.14585 | 0.38913 | |
Na+ | Spearman Corr. | 0.31516 | 0.21767 | 0.1703 | 1 | 0.2719 | 0.30463 | -0.17715 | 0.02277 | -0.00193 |
p-value | 0.00661 | 0.06432 | 0.14973 | -- | 0.01996 | 0.00927 | 0.13379 | 0.84837 | 0.98704 | |
K+ | Spearman Corr. | 0.20939 | 0.03685 | 0.33751 | 0.2719 | 1 | 0.33404 | -0.20051 | 0.11415 | 0.01169 |
p-value | 0.07542 | 0.75693 | 0.0035 | 0.01996 | -- | 0.00413 | 0.08897 | 0.33624 | 0.92183 | |
Cl- | Spearman Corr. | 0.19574 | 0.31182 | 0.03016 | 0.30463 | 0.33404 | 1 | -0.19869 | 0.17667 | -0.02442 |
p-value | 0.09939 | 0.00767 | 0.80144 | 0.00927 | 0.00413 | -- | 0.09429 | 0.13767 | 0.83866 | |
HCO3 | Spearman Corr. | -0.09797 | 0.06046 | 0.13798 | -0.17715 | -0.20051 | -0.19869 | 1 | -0.39045 | 0.40931 |
p-value | 0.40961 | 0.61137 | 0.24438 | 0.13379 | 0.08897 | 0.09429 | -- | 6.37658E-4 | 3.23599E-4 | |
Serum Creatinine | Spearman Corr. | 0.16848 | -0.13672 | -0.17192 | 0.02277 | 0.11415 | 0.17667 | -0.39045 | 1 | -0.70066 |
p-value | 0.15419 | 0.24875 | 0.14585 | 0.84837 | 0.33624 | 0.13767 | 6.37658E-4 | -- | <0.0001 | |
GFR | Spearman Corr. | -0.23618 | 0.18751 | 0.1023 | -0.00193 | 0.01169 | -0.02442 | 0.40931 | -0.70066 | 1 |
p-value | 0.04426 | 0.11217 | 0.38913 | 0.98704 | 0.92183 | 0.83866 | 3.23599E-4 | <0.0001 | -- | |
2-tailed test of significance is used | ||||||||||
PCA | Principal Component Analysis |
SC | Serum Creatinine |
eGFR | Estimated Glomerular Filtration Rate |
DF | Diabetic Foot |
DFU | Diabetic Foot Ulcers |
RA | Regional Anesthesia |
AB | Ankle Block |
ESRD | End Stage Renal Disease |
DCM | Dilated Cardio Myopathy |
RL | Resource-limited |
STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
RF | Renal Function |
SA | Serum Albumin |
CR | Cardio-Renal |
EB | Electrolyte Balance |
MA | Metabolic Acidosis |
CKD | Chronic Kidney Disease |
HR | High Risk |
| [1] | Hosseinzadeh P, Djazayery A, Mostafavi SA, Javanbakht MH, Derakhshanian H, Rahimiforoushani A, et al. Brewer’s yeast improves blood pressure in Type 2 diabetes mellitus. PubMed. 2013 Jan 1; 42(6): 602–9. Available from: |
| [2] | Coman LI, Ianculescu M, Paraschiv EA, Alexandru A, Bădărău IA. Smart solutions for Diet-Related Disease Management: connected care, remote health monitoring systems, and integrated insights for advanced evaluation. Applied Sciences. 2024 Mar 11; 14(6): 2351. Available from: |
| [3] | Mo M, Huang Z, Huo D, Pan L, Xia N, Liao Y, et al. Influence of Red Blood Cell Distribution Width on All-Cause Death in Critical Diabetic Patients with Acute Kidney Injury. Diabetes Metabolic Syndrome and Obesity. 2022 Aug 1; Volume 15: 2301–9. Available from: |
| [4] | Mohiuddin AK. TRACK Implementation: a Bangladesh Scenario. Central Asian Journal of Global Health. 2020 May 26; 9(1): e416. Available from: |
| [5] | Bai M, Sun X, Tan X, Gao Y. Editorial: Metabolic diseases and healthy aging: prevention and public health policy based on risk factors. Frontiers in Public Health. 2024 Oct 22; 12: 1502564. Available from: |
| [6] | Shim DW, Lee W, Park KH, Yoon YK, Park M, Park S, et al. Risk factors and mortality for amputations in the diabetic foot: a nationwide cohort study. Diabetes Research and Clinical Practice. 2025 Aug 23; 234: 112435. Available from: |
| [7] | Pearce CJ, Hamilton PD. Current concepts review: Regional Anesthesia for foot and ankle surgery. Foot & Ankle International. 2010 Aug 1; 31(8): 732–9. Available from: |
| [8] | Tran DQ, Salinas FV, Benzon HT, Neal JM. Lower extremity regional anesthesia: essentials of our current understanding. Regional Anesthesia & Pain Medicine. 2019 Jan 11; 44(2): 143–80. Available from: |
| [9] | Centria-Ammattikorkeakoulu. PROPER GLYCEMIC CONTROL OF ADULT DIABETIC PATIENT IN PERIOPERATIVE NURSING CARE. : A LITERATURE REVIEW.. Theseus. 2015. Available from: |
| [10] | Kir MC, Kir G. Ankle nerve block adjuvant to general anesthesia reduces postsurgical pain and improves functional outcomes in hallux valgus surgery. Medical Principles and Practice. 2018 Jan 1; 27(3): 236–40. Available from: |
| [11] | Wang A, Lv G, Cheng X, Ma X, Wang W, Gui J, et al. Guidelines on multidisciplinary approaches for the prevention and management of diabetic foot disease (2020 edition). Burns & Trauma. 2020 Jan 1; 8: tkaa017. Available from: |
| [12] | Pascarella G, De Quattro E, Strumia A, Del Buono R, Gargano F, Ruggiero A, et al. Perioperative analgesia for foot and ankle surgery: A Comprehensive review. Journal of Clinical Medicine. 2025 Sep 6; 14(17): 6301. Available from: |
| [13] | Roy SK, Dipu, Parveen R, Islam T, Aman A, Ullah MM, et al. Evaluating risk factors and surgical outcomes in diabetic foot patients at a tertiary care hospital. International Journal of Community Medicine and Public Health. 2025 Sep 30; 12(10): 4335–40. Available from: |
| [14] | Afroz SS, Das A, Kaiser MS. Risk factors associated with adverse outcomes in patients with diabetic foot infection in a tertiary hospital in Chattogram. Journal of Chittagong Medical College Teachers Association. 2025 Aug 25; 35(1): 127–34. Available from: |
| [15] | Akhtar S, Nasir JA, Sarwar A, Nasr N, Javed A, Majeed R, et al. Prevalence of diabetes and pre-diabetes in Bangladesh: a systematic review and meta-analysis. BMJ Open. 2020 Sep 1; 10(9): e036086. Available from: |
| [16] | Foster AVM. Multidisciplinary care of the diabetic foot. Journal of Wound Care. 1997 Apr 1; 6(Sup4): 21–4. Available from: |
| [17] | Levy N, Lirk P. Regional anaesthesia in patients with diabetes. Anaesthesia. 2021 Jan 1; 76(S1): 127–35. Available from: |
| [18] | Palialexi L, Makris A, Tsirogianni A, Zisopoulou V, Mania Th. Ankle block for foot surgery in high-risk patients. Regional Anesthesia & Pain Medicine. 2007 Sep 1; 32(Suppl. 1): 121. Available from: |
| [19] | Vandenbroucke JP, Von Elm E, Altman DG, Gøtzsche PC, Mulrow CD, Pocock SJ, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. International Journal of Surgery. 2014 Jul 18; 12(12): 1500–24. Available from: |
| [20] | Hensgens KRC, Van Rensen IHT, Lekx AW, Van Osch FHM, Knarren LHH, Wyers CE, et al. Sort and Sieve: Pre-Triage Screening of Patients with Suspected COVID-19 in the Emergency Department. International Journal of Environmental Research and Public Health. 2021 Sep 2; 18(17): 9271. Available from: |
| [21] | Zhu G, Xu J, Dai H, Min D, Guo G. Effect of peripheral nerve block versus general anesthesia on the hemodynamics and prognosis of diabetic patients undergoing diabetic foot Surgery. Diabetology & Metabolic Syndrome. 2023 Oct 26; 15(1): 213. Available from: |
| [22] | Galofaro E, D’Antonio E, Patané F, Casadio M, Masia L. Three-Dimensional assessment of upper limb proprioception via a wearable exoskeleton. Applied Sciences. 2021 Mar 15; 11(6): 2615. Available from: |
| [23] | Caravaca F, Arrobas M, Pizarro JL, Espárrago JF. serum albumin in advanced renal failure: Differences between diabetic and nondiabetic patients. American Journal of Kidney Diseases. 1999 May 1; 33(5): 892–8. Available from: |
| [24] | Adamczak M, Masajtis-Zagajewska A, Mazanowska O, Madziarska K, Stompór T, Więcek A. Diagnosis and Treatment of Metabolic Acidosis in Patients with Chronic Kidney Disease – Position Statement of the Working Group of the Polish Society of Nephrology. Kidney & Blood Pressure Research. 2018 Jan 1; 43(3): 959–69. Available from: |
| [25] | Nagami GT, Hamm LL. Regulation of Acid-Base balance in chronic kidney Disease. Advances in Chronic Kidney Disease. 2017 Sep 1; 24(5): 274–9. Available from: |
| [26] | Kuhn C, Mohebbi N, Ritter A. Metabolic acidosis in chronic kidney disease: mere consequence or also culprit? Pflügers Archiv - European Journal of Physiology. 2024 Jan 27; 476(4): 579–92. Available from: |
| [27] | Machado AD, Marchioni DM, Lotufo PA, Benseñor IM, Titan SM. Dietary acid load and the risk of events of mortality and kidney replacement therapy in people with chronic kidney disease: the Progredir Cohort Study. European Journal of Clinical Nutrition. 2023 Oct 27; 78(2): 128–34. Available from: |
| [28] | Kraut JA, Madias NE. Metabolic Acidosis of CKD: an update. American Journal of Kidney Diseases. 2015 Oct 26; 67(2): 307–17. Available from: |
| [29] | Korus J, Gołębiowski M, Stojanowski J, Szymczak M, Żabińska M, Bartoszek D, et al. The ratio of chloride to bicarbonate is a predictor of advanced metabolic acidosis in CKD stages G4 and G5. Scientific Reports. 2025 Jun 6; 15(1): 19958. Available from: |
| [30] | Koch CA, Fulop T. Clinical aspects of changes in water and sodium homeostasis in the elderly. Reviews in Endocrine and Metabolic Disorders. 2017 Mar 1; 18(1): 49–66. Available from: |
| [31] | Merkusheva LI, Runikhina NK, Tkacheva ON. Kidney aging. Geriatric view. Russian Journal of Geriatric Medicine. 2021 Apr 19; (1): 76–81. Available from: |
| [32] | Park SE, Ko SH, Kim JY, Kim K, Moon JH, Kim NH, et al. Diabetes fact sheets in Korea 2024. Diabetes & Metabolism Journal. 2025 Jan 1; 49(1): 24–33. Available from: |
| [33] | Kleinová P, Tímea B, Matej V, Graňák K, Andrej K, Katarína Š, et al. Nutritional and Metabolic Interventions to Prevent and Treat Protein–Energy Wasting in Nondialysis CKD—Narrative review. Nutrients. 2026 Jan 24; 18(3): 390. Available from: |
| [34] | Gregg LP, Carmody T, Le D, Martins G, Trivedi M, Hedayati SS. A Systematic Review and Meta-Analysis of Depression and Protein–Energy wasting in kidney Disease. Kidney International Reports. 2019 Dec 21; 5(3): 318–30. Available from: |
| [35] | Soliman DIMD; D MD, Abass F MD. Changes in kidney function (GFR), albuminuria, electrolytes, and heart affection in diabetic chronic kidney disease patients. The Medical Journal of Cairo University/˜the œMedical Journal of Cairo University. 2021 Dec 1; 89(12): 2923–33. Available from: |
| [36] | Kraut JA, Madias NE. Metabolic acidosis: pathophysiology, diagnosis and management. Nature Reviews Nephrology. 2010 Mar 23; 6(5): 274–85. Available from: |
| [37] | Kraut JA, Madias NE. Adverse effects of the metabolic acidosis of chronic kidney disease. Advances in Chronic Kidney Disease. 2017 Sep 1; 24(5): 289–97. Available from: |
| [38] | D’Souza D, Empringham J, Pechlivanoglou P, Uleryk EM, Cohen E, Shulman R. Incidence of diabetes in children and adolescents during the COVID-19 pandemic. JAMA Network Open. 2023 Jun 30; 6(6): e2321281. Available from: |
| [39] | Kutlugun AA, Yildiz C, Ebinc FA. Frequency of hyperkalemia in chronıc kidney patients under regular nephrology care. Journal of Clinical Nephrology and Renal Care. 2017 Nov 3; 3(2). Available from: |
| [40] | Melamed ML, Horwitz EJ, Dobre MA, Abramowitz MK, Zhang L, Lo Y, et al. Effects of sodium bicarbonate in CKD stages 3 and 4: A randomized, Placebo-Controlled, multicenter clinical trial. American Journal of Kidney Diseases. 2019 Nov 5; 75(2): 225–34. Available from: |
| [41] | Ossai CI, Wickramasinghe N. A hybrid approach for risk stratification and predictive modelling of 30-days unplanned readmission of comorbid patients with diabetes. Journal of Diabetes and Its Complications. 2022 Apr 20; 36(6): 108200. Available from: |
| [42] | Chatterjee R, Kwee LC, Pagidipati N, Koweek LH, Mettu PS, Haddad F, et al. Multi-dimensional characterization of prediabetes in the Project Baseline Health Study. Cardiovascular Diabetology. 2022 Jul 18; 21(1): 134. Available from: |
| [43] | Chen H, Su X, Li Y, Dang C, Luo Z. Identification of metabolic reprogramming-related genes as potential diagnostic biomarkers for diabetic nephropathy based on bioinformatics. Diabetology & Metabolic Syndrome. 2024 Nov 28; 16(1): 287. Available from: |
| [44] | Li X, Liang Q, Zhong J, Gan L, Zuo L. The effect of metabolic syndrome and its individual components on renal function: A Meta-Analysis. Journal of Clinical Medicine. 2023 Feb 17; 12(4): 1614. Available from: |
| [45] | Zhang C, Li H, Wang S. Common gene signatures and molecular mechanisms of diabetic nephropathy and metabolic syndrome. Frontiers in Public Health. 2023 Mar 30; 11: 1150122. Available from: |
| [46] | O’Sullivan ED, Hughes J, Ferenbach DA. Renal aging: causes and consequences. Journal of the American Society of Nephrology. 2016 Nov 15; 28(2): 407–20. Available from: |
APA Style
Tanzil, T., Islam, M. M., Bani, M. M. A. (2026). Cardio-renal and Metabolic Comorbidity Clusters in High-Risk Diabetic Patients Selected for Ankle Block Anesthesia: A Retrospective Correlational Analysis. International Journal of Anesthesia and Clinical Medicine, 14(2), 115-126. https://doi.org/10.11648/j.ijacm.20261402.11
ACS Style
Tanzil, T.; Islam, M. M.; Bani, M. M. A. Cardio-renal and Metabolic Comorbidity Clusters in High-Risk Diabetic Patients Selected for Ankle Block Anesthesia: A Retrospective Correlational Analysis. Int. J. Anesth. Clin. Med. 2026, 14(2), 115-126. doi: 10.11648/j.ijacm.20261402.11
@article{10.11648/j.ijacm.20261402.11,
author = {Tasnuva Tanzil and Md. Mazharul Islam and Md. Mostafa Al Bani},
title = {Cardio-renal and Metabolic Comorbidity Clusters in
High-Risk Diabetic Patients Selected for Ankle Block Anesthesia: A Retrospective Correlational Analysis},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {2},
pages = {115-126},
doi = {10.11648/j.ijacm.20261402.11},
url = {https://doi.org/10.11648/j.ijacm.20261402.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261402.11},
abstract = {Patients with diabetic foot often have multiple cardio-renal and metabolic comorbidities, which increase perioperative risk, especially in resource-limited settings where ankle block anesthesia is commonly used. The aim of the present study was to identify clusters of these comorbidities in high-risk diabetic patients undergoing foot surgery with ankle block anesthesia and to study correlations among key clinical parameters relevant to perioperative risk. A retrospective correlational study was performed on 71 adult diabetic patients who underwent foot surgery with ankle block anesthesia at Diabetic General Hospital, Chattogram, Bangladesh. Demographic and clinical data, encompassing biochemical, haematologic, renal, and cardiac parameters, were obtained from hospital records. Spearman's rank correlation, principal component analysis (PCA), and hierarchical clustering were used to find patterns of multimorbidity. There were strong links between renal and metabolic variables. Serum creatinine (SC) exhibited a robust inverse correlation with estimated glomerular filtration rate (eGFR), whereas bicarbonate showed a negative correlation with creatinine, indicating a potential link between metabolic acidosis and renal dysfunction. Positive correlations between electrolytes, albumin, and hemoglobin signify homeostatic equilibrium. PCA identified two principal axes-metabolic-electrolyte integrity and renal dysfunction-that encompassed the majority of the variance. Hierarchical clustering delineated three distinct physiological groupings. These results emphasize the necessity for thorough preoperative assessment and multidisciplinary management to enhance perioperative outcomes in this high-risk population. Prospective studies are necessary to enhance risk assessment methodologies.},
year = {2026}
}
TY - JOUR T1 - Cardio-renal and Metabolic Comorbidity Clusters in High-Risk Diabetic Patients Selected for Ankle Block Anesthesia: A Retrospective Correlational Analysis AU - Tasnuva Tanzil AU - Md. Mazharul Islam AU - Md. Mostafa Al Bani Y1 - 2026/07/03 PY - 2026 N1 - https://doi.org/10.11648/j.ijacm.20261402.11 DO - 10.11648/j.ijacm.20261402.11 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 115 EP - 126 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20261402.11 AB - Patients with diabetic foot often have multiple cardio-renal and metabolic comorbidities, which increase perioperative risk, especially in resource-limited settings where ankle block anesthesia is commonly used. The aim of the present study was to identify clusters of these comorbidities in high-risk diabetic patients undergoing foot surgery with ankle block anesthesia and to study correlations among key clinical parameters relevant to perioperative risk. A retrospective correlational study was performed on 71 adult diabetic patients who underwent foot surgery with ankle block anesthesia at Diabetic General Hospital, Chattogram, Bangladesh. Demographic and clinical data, encompassing biochemical, haematologic, renal, and cardiac parameters, were obtained from hospital records. Spearman's rank correlation, principal component analysis (PCA), and hierarchical clustering were used to find patterns of multimorbidity. There were strong links between renal and metabolic variables. Serum creatinine (SC) exhibited a robust inverse correlation with estimated glomerular filtration rate (eGFR), whereas bicarbonate showed a negative correlation with creatinine, indicating a potential link between metabolic acidosis and renal dysfunction. Positive correlations between electrolytes, albumin, and hemoglobin signify homeostatic equilibrium. PCA identified two principal axes-metabolic-electrolyte integrity and renal dysfunction-that encompassed the majority of the variance. Hierarchical clustering delineated three distinct physiological groupings. These results emphasize the necessity for thorough preoperative assessment and multidisciplinary management to enhance perioperative outcomes in this high-risk population. Prospective studies are necessary to enhance risk assessment methodologies. VL - 14 IS - 2 ER -
Department of Anesthesia, Chittagong Medical College Hospital, Chittagong, Bangladesh
Department of Nautical Science, Marine Fisheries Academy, Chittagong, Bangladesh
Department of Orthopedic, Chittagong Medical College Hospital, Chittagong, Bangladesh
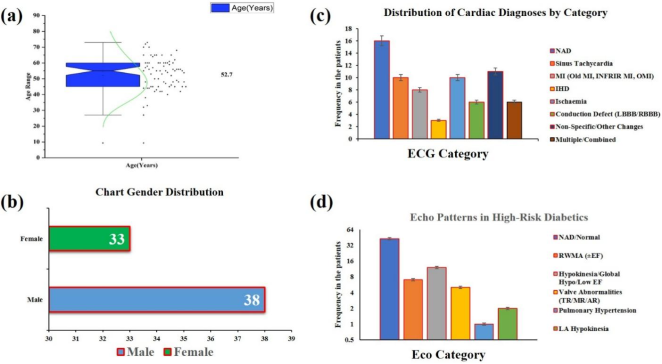
Figure 1. Clinical characteristics of the study population: (a) Age distribution with box-plot and density curve; (b) Gender distribution; (c) Distribution of electrocardiographic diagnostic categories; and (d) Echocardiographic patterns among high-risk diabetic patients.
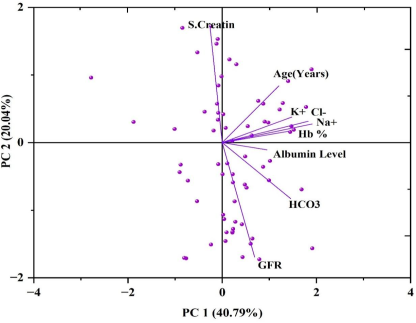
Figure 2. Principal component analysis revealing two distinct comorbidity clusters. Cluster 1 (PC1, 40.79%): Metabolic-electrolyte variables including Na⁺, Cl⁻, K⁺, HCO₃⁻, Hb%, albumin, and age. Cluster 2 (PC2, 20.04%): Renal function markers with creatinine opposing GFR and bicarbonate. Together, these components explain 60.83% of the total variance in the dataset.
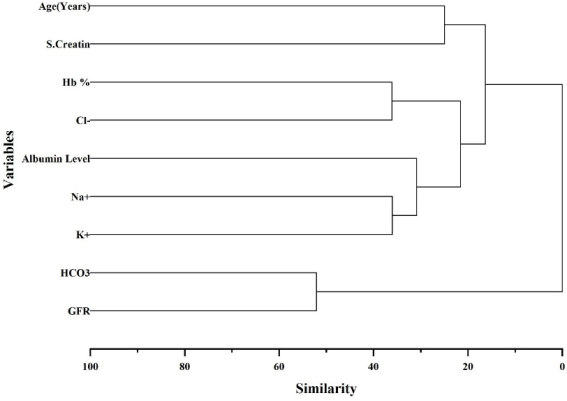
Figure 3. Multidimensional Comorbidity Clusters in Diabetic Patients: A Cardio-Renal-Metabolic Perspective.
Information

